|

|
|
|
|
|
This article may be reprinted free of charge provided 1) that there is clear attribution to the Orthomolecular Medicine News Service, and 2) that both the OMNS free subscription link http://orthomolecular.org/subscribe.html and also the OMNS archive link http://orthomolecular.org/resources/omns/index.shtml are included. FOR IMMEDIATE RELEASE
A Hallmark of Covid-19: Cytokine Storm/Oxidative Stress and its Integrative Mechanism
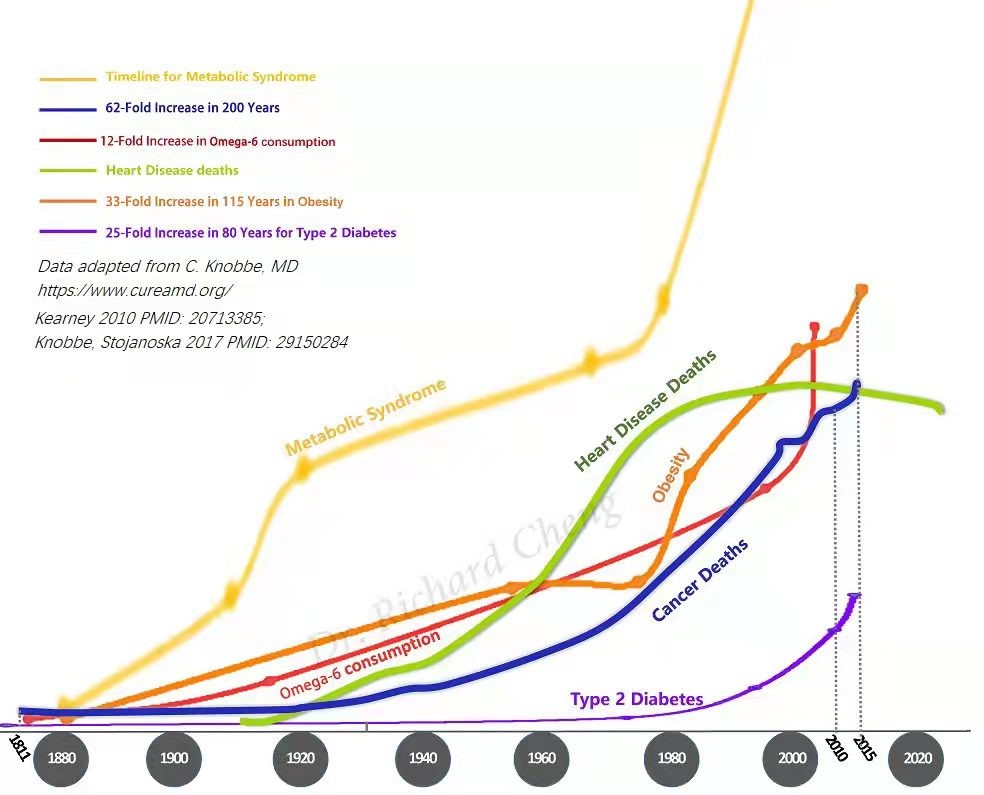
by Richard Z. Cheng, M.D., Ph.D.OMNS (Jan. 22, 2022) Cytokine storm has recently been recognized as the key pathology responsible for the severe symptoms of Covid-19 and other viruses and non-viral agents. The underlying biochemical cause of cytokine storm is excessive oxidative stress. Cytokine storm and its associated oxidative stress appears to be a universal non-specific mechanistic pathway common among many causative agents, for example viruses, that leads to severe clinical disease. A biochemical sequence known as "lipid peroxidase chain reaction" (LPCR) plays a critical role in oxidative stress and cytokine storm. Prevention and blocking the occurrence of cytokine storm/oxidative stress appears to be a logically sound and effective strategy to prevent the severe symptoms of Covid-19. If this could be performed world-wide, it could reduce the devastating medical, economic and societal impact of the Covid-19 pandemic. Preventing or blocking LPCR and the excessive oxidative stress requires intact antioxidant systems, especially the antioxidant vitamins and nutrients, including vitamins C, E, CoQ10, alpha lipoic acid, glutathione and niacin (to promote NADP+/NADP), selenium and others. Insufficiency or absence of any of these antioxidant agents may render these antioxidant systems ineffective, which may be responsible for the inconsistent results of antioxidant therapies in the literature. Here we propose an integrative and systematic therapy that includes these antioxidant vitamins, minerals, and nutrients. The "universal and non-specific nature" of cytokine storm/oxidative stress makes possible a pre-emptive treatment to prevent or block cytokine storm/oxidative stress induced by severe diseases, even before full recognition of the underlying causative agent. This is very significant because it allows us to potentially prevent and block a pandemic of a new virus or a new viral mutant when it happens without requiring the extended time needed to develop a specific drug or vaccine treatment. With the seemingly endless mutations of SARS-Cov-2, we may still have time to apply this strategy to break the Covid-19 pandemic. A key hallmark of Covid-19: Cytokine storm/oxidative stressCytokine storm with the underlying elevated oxidative stress is a key hallmark of severe Covid-19. [1-12] Cytokine storm was first described 28 years ago [13,14] and is a common mechanism leading to severe symptoms, not only in Covid-19, but also in other respiratory viral infections [15,16], HIV-related infections [17,18], sepsis [19], SARS [20], tick-borne SFTS syndrome [21], autoimmune and viral hepatitis [22,23], Ebola [24], yellow fever [25], and Coronaviral encephalitis [26], immunotherapies [27,28], as well as systemic diseases and anaphylaxis. [29] Cytokine storm describes the explosive and excessive release of free radicals and cytokines (signaling molecules) in a short period of time, overwhelming the body's innate antioxidant/anti-inflammatory mechanisms, leading to significant oxidative damage of biologically important molecules such as DNA, proteins and lipids, and severe cellular and organ damage. This can rapidly progress to multi-organ failure with a very high mortality rate. Hence, it is very important to recognize the early clinical signs of cytokine storm and prevent it from developing. If we can interrupt the cytokine storm/oxidative stress before it causes significant cellular and tissue damage, this will provide a way to prevent severe Covid-19 and other severe viral syndromes. One exciting possibility is to administer early and sufficient doses of antioxidants to strengthen the body's antioxidant defenses. This can play a major role in prevention and intervention of cytokine storm/oxidative stress. [5,6] Antioxidant vitamins and nutraceuticals have been used for this purpose in the management of Covid-19. Some of these nutrients showed significant effectiveness in treating Covid-19 [30-33], and "Long Covid" symptoms. [34] Lipid peroxidation plays a central and an important role in cytokine storm. Unlike oxidation of DNA and protein, lipid peroxidation is unique in that it usually happens rapidly, damaging many of the lipid molecules in a local cellular environment through a lipid peroxidation chain reaction (LPCR). It can continue until all the unsaturated lipid molecules in cell membranes are damaged or until LPCR is terminated by antioxidants, usually the body's main lipophilic antioxidant, vitamin E. [35-38] The prevention of lipid peroxidation and termination of LPCR requires a series of antioxidants to work together in a systematic manner, like a cogwheel. Lacking or insufficiency of any one component may render the entire antioxidant cascade ineffective. There is little recognition of this "integrative or systematic" working relationship in the literature. [35] This lack of recognition may be responsible for the failure of some antioxidant studies to show clinical effectiveness. The main purpose of this article is to analyze and present this "Integrative Antioxidant Therapies" concept. Cytokine storm/oxidative stress is a pathobiological response that can be induced by various pathogens and by nature is non-pathogen-specific. Thus therapeutic strategies to prevent or block cytokine storm/oxidative stress may be a very effective general method to prevent/treat diseases involving cytokine storm/oxidative stress. This point may have a wide-reaching clinical significance, especially in the current global management of Covid-19 pandemic. Despite the various causes that may induce a cytokine storm and the varied cytokine responses that may happen in a cytokine storm, the associated elevated oxidative stress response for any particular causative agent is very likely similar. This makes it possible to develop an antioxidant therapy to prevent or block the severe diseases that result from the cytokine storm, including severe Covid-19 pneumonia. One of the difficulties in developing preventive treatments for pandemics like Covid-19 is the rapid mutations of these RNA viruses. But with cytokine storm as the common feature of such severe diseases, it may be possible to prevent these severe diseases with integrative antioxidant therapies to prevent or block the cytokine storm, even without detailed studies of new virus mutants. This applies not only to Covid-19; it may be applicable to other future epidemics, and other severe viral diseases. The clinical, societal and economic impact of this strategy is so profound that further research is urgently needed with top priority. One of the key problems dealing with Covid-19 and other epidemic/pandemic-causing viruses is their rapid mutation rates, which can often obviate the few available virus specific vaccines and/or drugs. We propose an integrative viricidal and antioxidant therapy that may be universally applicable to Covid-19 and other viral infections, including various Covid-19 mutants and future mutants. Lipid peroxidation chain reaction (LPCR), a key cascade of events in cytokine storm:LPCR is well studied and established in the field of biochemistry. LPCR has 3 stages: the Initiation stage, the Propagation stage, and the final Termination stage. [39] LPCR not only damages lipid molecules, which make up the cell membrane, but the LPCR process also causes a number of very toxic oxidation products including lipid hydroperoxides (LOOH) and aldehydes such as malondialdehyde (MDA) and 4-hydroxynonenal (4-HNE). MDA is the most mutagenic product of lipid peroxidation and is commonly used as a biomarker for oxidative deterioration in omega-3 and omega-6 fatty acids. 4-HNE is the most toxic secondary product of lipid peroxidation. Lipid peroxidation chain reaction (LPCR) is at the center of the cytokine storm, producing free radicals. [36,40-43] In turn, free radicals oxidize and damage DNA, proteins and lipids. The oxidation of lipids is biochemically called peroxidation. Once a lipid molecule is oxidized (this is called initiation), it becomes a lipid radical. The lipid radical can oxidize the next lipid molecule in the neighborhood very readily and rapidly until this chain event is terminated by antioxidants, especially vitamin E. Lipid peroxidation has been implicated in the development and progression of critical illnesses. [43] High levels of lipid peroxidation are associated with severe Covid-19 symptoms. [44-46] Protein adducts of lipid peroxidation products (4-HNE) were found to be higher in patients who died of severe Covid-19 symptoms than in those who survived Covid-19. [47] Excessive oxidative stress is common in many, if not all, acute and chronic diseases, including Covid-19.Oxidative stress describes biochemical reactions involving reactive molecules, including reactive oxygen species (ROS) and reactive nitrogen species (RNS), sometimes collectively abbreviated as RONS. Oxidative stress is an important part of redox signaling inherent in cell physiology. [48-50] Lipid peroxidation is also implicated in many chronic diseases, such as cardiovascular disease [51-56], cancer [57-60], Alzheimer's, liver diseases, lung diseases (COPD), diabetes mellitus [61-68], autoimmune diseases [69-73], and also Covid-19, chronic Covid-19 symptoms (so-called "Long Covid") and even Covid vaccine related injuries. [5,34,47,74-84] More advanced atherosclerosis is found to be associated with increased oxidized linoleic acid (LA) than with non-oxidized LA. [85] Polyunsaturated fatty acids (PUFAs) are the targets of LPCR:LPCR primarily targets the double bonds in lipid molecules. PUFAs are the fatty acids with unsaturated double bonds between the carbon molecules in their backbone. Hence PUFAs are the primary targets of LPCR. All fatty acids can be oxidized, but with increasing difficulty from PUFAs to MUFAs (monounsaturated fatty acids) to saturated fats. [86] The double bonds in PUFAs are relatively unstable and can be readily broken by oxidative free radicals, causing damage to these lipids. Cell membranes, and the membrane of subcellular organelles such as mitochondria are made up mostly of lipids. Once these lipids are damaged, their functions are also impaired. Cardiolipin, e.g., an abundant lipid on the mitochondria membrane, plays a critical role in cellular energy production. Peroxidation of PUFAs in cardiolipin may contribute to age-related decline in the mitochondrial function. [86] Cardiolipin is found to be damaged in many cancer cells as well. [87-90] Saturated fatty acids don't have these double bonds, and MUFAs have only one such double bond. Hence saturated fats and MUFAs are more stable and less readily oxidized by free radicals. The amount of dietary omega-6 polyunsaturated fatty acids (N6 PUFAs) has increased significantly over the past few decades:Due to decades of widespread misinformation that saturated fats are unhealthy, the intake of unsaturated fats, especially in the form of N-6 rich seed oils has significantly increased in modern diets. [91-93] Although both N-3 and N-6 are essential fatty acids, N-6 PUFA has a pro-inflammation effect, while N-3 PUFA is anti-inflammatory. The N-6 to N-3 fatty acid ratio has increased significantly from a ratio of ~1:1 during prehistoric evolution to 20:1 or even higher in recent decades. The increased N6/N3 ratio has been found to be correlated with various chronic diseases. [39,91,93,94] Although the recent abnormally high N6/N3 ratio may not have a direct impact on LPCR and cytokine storm, the increased total PUFA in our body is a setup for potentially more explosive LPCR. These PUFAs are enriched in cell membranes [95] which allows the membranes to be more readily attacked by the free radicals. This happens especially in a cytokine storm, with a huge outburst of free radicals in a short period of time, which overwhelms the antioxidant capacity of cells, leading to the initiation and propagation of the lipid peroxidation chain reaction. This increase of dietary N-6 PUFA intake is especially found among those with metabolic diseases such as diabetes. [91-93] This may explain why patients with metabolic diseases are prone to severe Covid-19 diseases with a high risk of multiorgan failure and mortality.
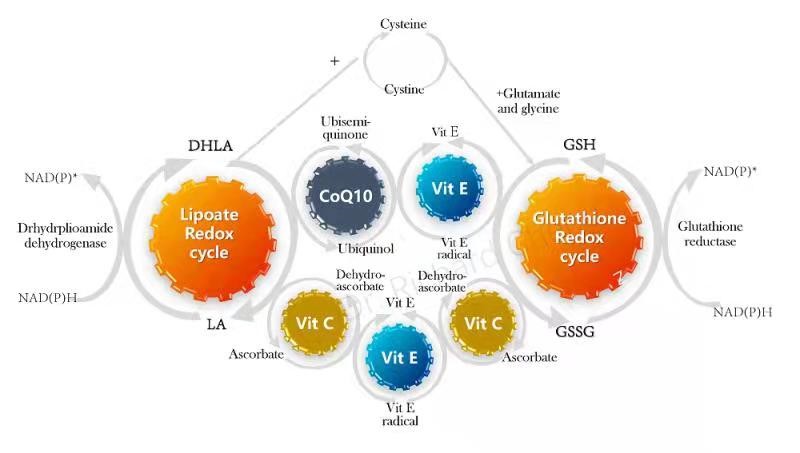
Termination of LPCR:Once LPCR is initiated, it can propagate until all the lipids are oxidized or until it is terminated by antioxidants, especially vitamin E (VE). [35,96-98] VE is the chief LPCR chain-breaking antioxidant. VE is a lipid soluble antioxidant vitamin and is located on cell membranes, sitting among the lipid molecules. These features make VE the key antioxidant vitamin to protect cell membranes from oxidation. Other antioxidants, such as vitamin C, the primary extracellular antioxidant, do not have this LCPR termination effect. [35] Cascade of Antioxidants:Vitamin E appears to be required to block the propagation of LPCR and to terminate LPCR. The oxidized VE will not in turn oxidize other lipid molecules, but instead, oxidized VE needs to be reduced by other antioxidants, especially vitamin C (VC). The oxidized VC needs to be reduced by alpha lipoic acid, CoQ10, glutathione, selenium and NADP+/NADP. The free radicals will be passed down onto NADP/NADPH cascade to be disposed of in water. These antioxidants work in a systematic manner (Fig. 2).
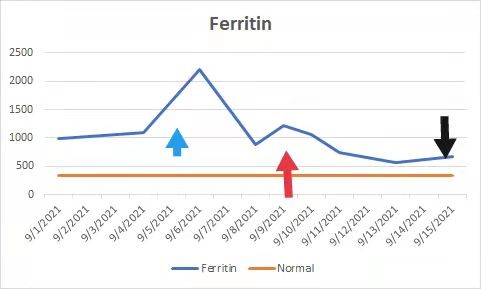
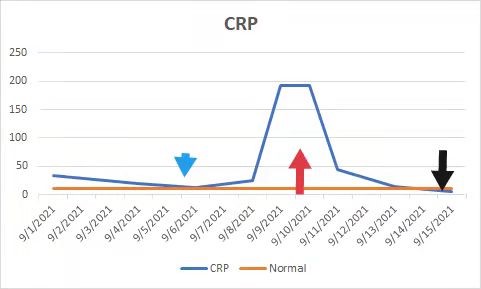
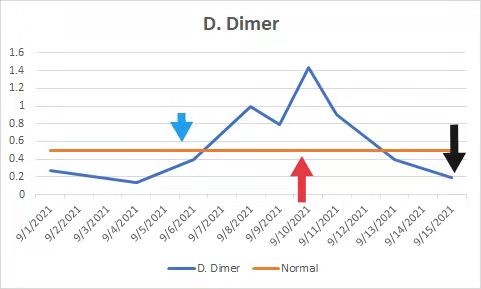
Systematic and integrative nature of the antioxidant systems:It should be noted that these antioxidants work in an integrative and systematic manner like a system of cogwheels. Each and every one of the components is required. It's been shown that in the absence of VE, VC is not able to prevent lipids from being attacked by LPCR. Sato et al. described in their study of LDP cholesterol that VE and VC together can prevent LDL oxidation. However, in the absence of VE, VC is unable to prevent the LDL oxidation. [35] A recent national survey found alarming high rates of vitamin deficiency among American adults: 45% of American adults are deficient in vitamin A, vitamin C (46% deficient), vitamin D (95% deficient), vitamin E (84% deficient) and zinc (15% deficient). [99] It is conceivable that when individuals deficient in antioxidant vitamins and nutrients are hit by cytokine storm, their innate LPCR prevention and termination mechanisms are severely impaired so they will suffer high rates of cytokine storm/oxidative stress damages, leading to severe diseases and death. Antioxidation therapies of various single antioxidants or a combination of a selected few antioxidants have been used to clinically treat various diseases. The results have been mixed. Lack of understanding of this "integrative and systematic" nature of antioxidant cascade may be responsible for at least some of the failures observed in those clinical antioxidant studies. The contribution of N-6 PUFA, LPCR, and the integrative nature of antioxidants in the prevention and termination of LPCR has not been previously addressed. To the best of my knowledge, this is the first time this concept is described. In fact, clinical attention of oxidation has been mostly given to DNA mutation, but hardly any attention has been given to the peroxidation of lipids and ways to prevent this life-threatening condition. Systematic Antioxidant TherapyThe terms cytokine storm and oxidative stress are associated with many viral syndromes and other non-viral infections. Systematic Antioxidants Therapy may have wide clinical application, and deserves further clinical studies. In summary, cytokine storm and associated oxidative stress appear to be a common mechanistic pathway leading to severe clinical diseases caused by viruses and other non-viral agents, including Covid-19. Lipid peroxidation is a central part of the cytokine storm. Prevention of the lipid peroxidation chain reaction and its termination requires an integrative and systematic antioxidant cascade including sufficient doses of vitamin C, vitamin E, CoQ10, alpha lipoic acid, glutathione and NAD+/NADP+ and others. Lacking or insufficiency of any of these components may render the antioxidant cascade ineffective, resulting in failure to prevent/block cytokine storm/oxidative stress. This mechanism is universal and non-specific to causative agents. Epidemics and pandemics are on the rise, despite the significantly improved global economy and technology. [7] This "universal and non-specific nature" makes it possible for preemptive therapy to prevent or block cytokine storm induced severe diseases from happening, even before full recognition of the underlying causative agent. This is important, because it potentially allows us to prevent and block a pandemic of a new virus or a new viral mutant when it occurs, without spending the long time needed for specific drug or vaccine research and development. With the seemingly endless mutations of SARS-Cov-2, we may still have time to apply this strategy to break the Covid-19 pandemic. Based on the biochemistry and pathology, we recommend high doses and early administration of antioxidants. We recommend vitamin C; vitamin E , alpha lipoic acid, CoQ10, glutathione and other vitamins and nutrients such as B vitamins and mitochondrial nutrients. Vitamin B3 (niacin) is critical in NAD+ biogenesis. NAD+ is involved in the final step of scavenging of free radicals. The rapid recovery in the case presented below highlights this approach. We recently consulted on a case of severe Covid-19 in a patient who rapidly recovered after the administration of this Integrative Antioxidant Therapy, based on the above understanding and analysis. Robert from Manila, the Philippines, was of advanced age with multiple comorbidities including type 2 diabetes mellitus, hypertension, obesity and history of chronic hepatitis B. Robert was diagnosed of Covid-19 in September 2021, admitted to ICU and received standard Covid-19 care in the hospital for a week without improvement. Instead, his symptoms deteriorated with decrease of oxygen saturation progressed down to as low as 90-92% and rapidly rising cytokine storm markers of CRP, D. Dimer and ferritin (Fig. 3-5). The family requested my consultation and I recommended Integrative Antioxidant Therapy (Fig. 6). However, due to policy restrictions of the hospital, Robert did not receive my recommended protocol. His clinical conditions worsened with continued rise of cytokine storm markers (Fig. 3-5) and I was consulted again 4 days later. At that time, Robert was on a verge of or already in a cytokine storm and his risks of developing multiorgan failure were very high. I strongly urged the attending physician to implement the Integrative Antioxidant Therapy Protocol. Finally, Robert received the recommended protocol (Fig. 6). He rapidly improved on Day 2 after the implementation of the Protocol. He didn't need the supplemental oxygen on Day 3 to maintain adequate blood oxygen saturation. On Day 5, he was discharged to home care. I recommended continued integrative antioxidant therapy to ensure maximal repair of cellular and tissue oxidative damages and to prevent long term Covid-19 symptoms.
Fig. 3. Robert's ferritin levels during his hospitalization. Orange line: upper limit of normal range. Blue line: patient's ferritin values. Blue arrow: my recommendation of Integrative Antioxidant Therapy on my first consultation. Red arrow: implementation of Integrative Antioxidants Therapy. Black Arrow: discharge from hospital.
Fig. 4. Robert's CRP levels during his hospitalization. Orange line: upper limit of normal range. Blue line: patient's CRP values. Blue arrow: my recommendation of Integrative Antioxidant Therapy on my first consultation. Red arrow: implementation of Integrative Antioxidants Therapy. Black Arrow: discharge from hospital.
Fig. 5. Robert's D. Dimer levels during his hospitalization. Orange line: upper limit of normal range. Blue line: patient's D. Dimer values. Blue arrow: my recommendation of Integrative Antioxidant Therapy on my first consultation. Red arrow: implementation of Integrative Antioxidants Therapy. Black Arrow: discharge from hospital.
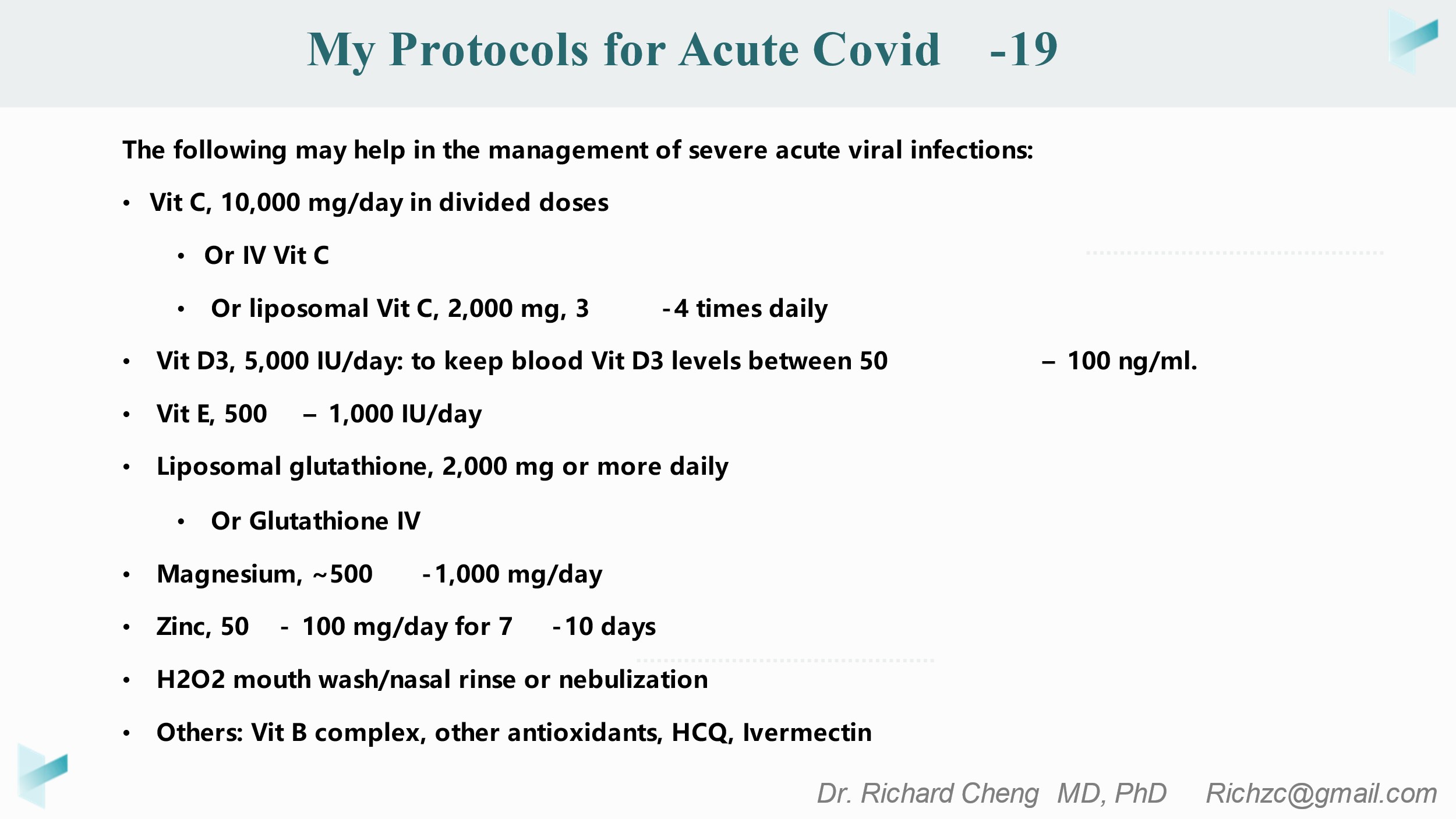
Fig. 6. Integrative Antioxidant Therapy Protocol (The following recommendations should be implemented under the supervision of a qualified healthcare provider):
ConclusionIn conclusion, oxidative stress plays a central role in severe Covid-19 diseases and other diseases involving cytokine storm and oxidative stress. Lipid peroxidation is a central part of the cytokine storm. The prevention and termination of the lipid peroxidation chain reaction requires an integrative and systematic antioxidant cascade including vitamin C, vitamin E, CoQ10, alpha lipoic acid, glutathione and NAD+/NADP+ and others. Lacking or insufficiency of any of these components may render the antioxidant cascade ineffective, resulting in failure to prevent/block cytokine storm/oxidative stress. This mechanism is universal and non-specific to pathogens. Recognition of this mechanism may have a wide clinical implication to many viral and non-viral diseases. Clearly further clinical studies are warranted. References1. Mulchandani R, Lyngdoh T, Kakkar AK. (2021) Deciphering the COVID-19 cytokine storm: Systematic review and meta-analysis. Eur J Clin Invest 51:e13429. https://pubmed.ncbi.nlm.nih.gov/33058143 2. Eljaaly K, Malibary H, Alsulami S, et al. (2021) Description and Analysis of Cytokine Storm in Registered COVID-19 Clinical Trials: A Systematic Review. Pathogens 10:692. https://pubmed.ncbi.nlm.nih.gov/34199506 3. Melo AKG, Milby KM, Caparroz ALMA, et al. (2021) Biomarkers of cytokine storm as red flags for severe and fatal COVID-19 cases: A living systematic review and meta-analysis. PLoS One 16:e0253894. https://pubmed.ncbi.nlm.nih.gov/34185801 4. Aucoin M, Cardozo V, McLaren MD, et al. (2021) A systematic review on the effects of Echinacea supplementation on cytokine levels: Is there a role in COVID-19? Metabol Open 11:100115. https://pubmed.ncbi.nlm.nih.gov/34341776 5. Cheng RZ. (2020) Can early and high intravenous dose of vitamin C prevent and treat coronavirus disease 2019 (COVID-19)? Medicine in Drug Discovery 5:100028. https://pubmed.ncbi.nlm.nih.gov/32328576 6. Cheng R, Kogan M, Devra D. (2020) Ascorbate as Prophylaxis and Therapy for COVID-19 -- Update From Shanghai and U.S. Medical Institutions. Glob Adv Health Med 9:2164956120934768. https://pubmed.ncbi.nlm.nih.gov/32733775 7. Cheng RZ (2020) Protected Population Immunity, Not A Vaccine, Is The Way To Stop Covid-19 Pandemic. J Clin Immunol Immunother 6:1-4. http://news.drwlc.com/Documents/HCIIT-20-011.pdf 8. Huang I, Pranata R, Lim MA, et al. (2020) C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: a meta-analysis. Ther Adv Respir Dis 14:1753466620937175. https://pubmed.ncbi.nlm.nih.gov/32615866 9. D'Errico S, Zanon M, Montanaro M, et al. (2020) More than Pneumonia: Distinctive Features of SARS-Cov-2 Infection. From Autopsy Findings to Clinical Implications: A Systematic Review. Microorganisms 8:1642. https://pubmed.ncbi.nlm.nih.gov/33114061 10. Olbei M, Hauteforte I, Modos D, et al. (2021) SARS-CoV-2 Causes a Different Cytokine Response Compared to Other Cytokine Storm-Causing Respiratory Viruses in Severely Ill Patients. Front Immunol 12:629193. https://pubmed.ncbi.nlm.nih.gov/33732251 11. Mosquera-Sulbaran JA, Pedreañez A, Carrero Y, Callejas D (2021) C-reactive protein as an effector molecule in Covid-19 pathogenesis. Rev Med Virol 31:e2221. https://pubmed.ncbi.nlm.nih.gov/34773448 12. Hu B, Huang S, Yin L (2021) The cytokine storm and COVID-19. J Med Virol 93:250-256. https://pubmed.ncbi.nlm.nih.gov/32592501 13. Ferrara JL, Abhyankar S, Gilliland DG (1993) Cytokine storm of graft-versus-host disease: a critical effector role for interleukin-1. Transplant Proc 25:1216-1217. https://pubmed.ncbi.nlm.nih.gov/8442093 14. Fajgenbaum DC, June CH (2020) Cytokine Storm. N Engl J Med 383:2255-2273. https://pubmed.ncbi.nlm.nih.gov/33264547 15. Khomich OA, Kochetkov SN, Bartosch B, Ivanov AV (2018) Redox Biology of Respiratory Viral Infections. Viruses 10:392. https://pubmed.ncbi.nlm.nih.gov/30049972 16. Oldstone MBA, Rosen H (2014) Cytokine storm plays a direct role in the morbidity and mortality from influenza virus infection and is chemically treatable with a single sphingosine-1-phosphate agonist molecule. Curr Top Microbiol Immunol 378:129-147. https://pubmed.ncbi.nlm.nih.gov/24728596 17. Parsi M, Dargan K (2020) Hemophagocytic Lymphohistiocytosis Induced Cytokine Storm Secondary to Human Immunodeficiency Virus Associated Miliary Tuberculosis. Cureus 12:e6589. https://pubmed.ncbi.nlm.nih.gov/32051801 18. Muema DM, Akilimali NA, Ndumnego OC, et al. (2020) Association between the cytokine storm, immune cell dynamics, and viral replicative capacity in hyperacute HIV infection. BMC Med 18:81. https://pubmed.ncbi.nlm.nih.gov/32209092 19. Chousterman BG, Swirski FK, Weber GF (2017) Cytokine storm and sepsis disease pathogenesis. Semin Immunopathol 39:517-528. https://pubmed.ncbi.nlm.nih.gov/28555385 20. Huang K-J, Su I-J, Theron M, et al. (2005) An interferon-gamma-related cytokine storm in SARS patients. J Med Virol 75:185-194. https://pubmed.ncbi.nlm.nih.gov/15602737 21. Sun Y, Jin C, Zhan F, et al. (2012) Host cytokine storm is associated with disease severity of severe fever with thrombocytopenia syndrome. J Infect Dis 206:1085-1094. https://pubmed.ncbi.nlm.nih.gov/22904342 22. Mbachu J, Bul V, Koppe SWP (2016) The Perfect (Cytokine) Storm: Autoimmune Hepatitis as a Catalyst for Macrophage Activation Syndrome: 1950. Am J Gastroenterol. 111:S930. https://journals.lww.com/ajg/Fulltext/2016/10001/The_Perfect__Cytokine__Storm__Autoimmune_Hepatitis.1950.aspx 23. Xie J, Wang M, Cheng A, et al. (2018) Cytokine storms are primarily responsible for the rapid death of ducklings infected with duck hepatitis A virus type 1. Sci Rep 8:6596. https://pubmed.ncbi.nlm.nih.gov/29700351 24. Younan P, Iampietro M, Nishida A, et al. (2017) Ebola Virus Binding to Tim-1 on T Lymphocytes Induces a Cytokine Storm. mBio 8:e00845-17. https://pubmed.ncbi.nlm.nih.gov/28951472 25. Monath TP (2008) Treatment of yellow fever. Antiviral Res 78:116-124. https://pubmed.ncbi.nlm.nih.gov/18061688 26. Savarin C, Bergmann CC (2018) Fine Tuning the Cytokine Storm by IFN and IL-10 Following Neurotropic Coronavirus Encephalomyelitis. Front Immunol 9:3022. https://pubmed.ncbi.nlm.nih.gov/30619363 27. Morgan RA, Yang JC, Kitano M, et al. (2010) Case report of a serious adverse event following the administration of T cells transduced with a chimeric antigen receptor recognizing ERBB2. Mol Ther 18:843-851. https://pubmed.ncbi.nlm.nih.gov/20179677 28. Hansel TT, Kropshofer H, Singer T, et al. (2010) The safety and side effects of monoclonal antibodies. Nat Rev Drug Discov 9:325-338. https://pubmed.ncbi.nlm.nih.gov/20305665 29. Lukan, N. (2020) "Cytokine storm", not only in COVID-19 patients. Mini-review. Immunol Lett 228:38-44. https://pubmed.ncbi.nlm.nih.gov/33007369 30. Colunga Biancatelli RML, Berrill M, Catravas JD, Marik PE (2020) Quercetin and Vitamin C: An Experimental, Synergistic Therapy for the Prevention and Treatment of SARS-CoV-2 Related Disease (COVID-19). Front Immunol 11:1451. https://pubmed.ncbi.nlm.nih.gov/32636851 31. Holford P, Carr AC, Jovic TH, et al. (2020) Vitamin C-An Adjunctive Therapy for Respiratory Infection, Sepsis and COVID-19. Nutrients 12:3760. https://pubmed.ncbi.nlm.nih.gov/33297491 32. Alexander J, Tinkov A, Strand TA, et al. (2020) Early Nutritional Interventions with Zinc, Selenium and Vitamin D for Raising Anti-Viral Resistance Against Progressive COVID-19. Nutrients 12:2358. https://pubmed.ncbi.nlm.nih.gov/32784601 33. Corrao S, Bocchio RM, Lo Monaco M, et al. (2021) Does Evidence Exist to Blunt Inflammatory Response by Nutraceutical Supplementation during COVID-19 Pandemic? An Overview of Systematic Reviews of Vitamin D, Vitamin C, Melatonin, and Zinc. Nutrients 13:1261. https://pubmed.ncbi.nlm.nih.gov/33921297 34. Vollbracht C, Kraft K (2021) Feasibility of Vitamin C in the Treatment of Post Viral Fatigue with Focus on Long COVID, Based on a Systematic Review of IV Vitamin C on Fatigue. Nutrients 13:1154. https://pubmed.ncbi.nlm.nih.gov/33807280 35. Sato K, Niki E, Shimasaki H (1990) Free radical-mediated chain oxidation of low density lipoprotein and its synergistic inhibition by vitamin E and vitamin C. Arch Biochem Biophys 279:402-405. https://pubmed.ncbi.nlm.nih.gov/2350187 36. Ayala A, Muñoz MF, Argüelles S (2014) Lipid peroxidation: production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxid Med Cell Longev 2014:360438. https://pubmed.ncbi.nlm.nih.gov/24999379 37. Niki E (1987) Antioxidants in relation to lipid peroxidation. Chem Phys Lipids 44:227-253. https://pubmed.ncbi.nlm.nih.gov/3311418 38. Babbs CF, Steiner MG (1990) Simulation of free radical reactions in biology and medicine: a new two-compartment kinetic model of intracellular lipid peroxidation. Free Radic Biol Med 8:471-485. https://pubmed.ncbi.nlm.nih.gov/2174816 39. Patterson E, Wall R, Fitzgerald GF, et al. (2012) Health Implications of High Dietary Omega-6 Polyunsaturated Fatty Acids. J Nutr Metab 2012:539426. https://pubmed.ncbi.nlm.nih.gov/22570770 40. Jancic S, et al. (2021) Lipid Peroxidation - an overview. ScienceDirect Topics. https://www.sciencedirect.com/topics/neuroscience/lipid-peroxidation 41. Repetto M, Semprine J, Boveris A (2012) Lipid Peroxidation: Chemical Mechanism, Biological Implications and Analytical Determination. Chapter 1 in: Catala A, Ed., Lipid Peroxidation, IntechOpen, 2012, ISBN-13: 978-9535107163. http://doi.org/10.5772/45943 42. Hassan HA, El-Aal MA (2012) Lipid Peroxidation End-Products as a Key of Oxidative Stress: Effect of Antioxidant on Their Production and Transfer of Free Radicals. Chapter 3 in: Catala A, Lipid Peroxidation, InTech: Rijeka, Croatia, 2012; pp. 63-88. ISBN-13: 978-9535107163. http://doi.org/10.5772/45944 43. Su L-J, Zhang J-H, Gomez H, et al. (2019) Reactive Oxygen Species-Induced Lipid Peroxidation in Apoptosis, Autophagy, and Ferroptosis. Oxid Med Cell Longev 2019:5080843. https://pubmed.ncbi.nlm.nih.gov/31737171 44. Potje SR, Costa TJ, Fraga-Silva TFC, et al. (2021) Heparin prevents in vitro glycocalyx shedding induced by plasma from COVID-19 patients. Life Sci 276:119376. https://pubmed.ncbi.nlm.nih.gov/33781826 45. Martín-Fernández M, Aller R, Heredia-Rodríguez M, et al. (2021) Lipid peroxidation as a hallmark of severity in COVID-19 patients. Redox Biology 48:102181. https://pubmed.ncbi.nlm.nih.gov/34768063 46. Laforge M, Elbim C, Frère C, et al. (2020) Tissue damage from neutrophil-induced oxidative stress in COVID-19. Nat Rev Immunol 20:515-516. https://pubmed.ncbi.nlm.nih.gov/32728221 47. Žarkovic N, Orehovec B, Milkovic L, et al. (2021) Preliminary Findings on the Association of the Lipid Peroxidation Product 4-Hydroxynonenal with the Lethal Outcome of Aggressive COVID-19. Antioxidants (Basel) 10:1341. https://pubmed.ncbi.nlm.nih.gov/34572973 48. Flohé, L. (2020) Looking Back at the Early Stages of Redox Biology. Antioxidants (Basel) 9:1254. https://pubmed.ncbi.nlm.nih.gov/33317108 49. Sies, H. (2017) Hydrogen peroxide as a central redox signaling molecule in physiological oxidative stress: Oxidative eustress. Redox Biol 11:613-619. https://pubmed.ncbi.nlm.nih.gov/28110218 50. Sies H, Berndt C, Jones DP (2017) Oxidative Stress. Annu Rev Biochem 86:715-748. https://pubmed.ncbi.nlm.nih.gov/28441057 51. Kattoor AJ, Pothineni NVK, Palagiri D, Mehta JL (2017) Oxidative Stress in Atherosclerosis. Curr Atheroscler Rep 19:42. https://pubmed.ncbi.nlm.nih.gov/28921056 52. Jenkins DJA, Kitts D, Giovannucci EL, et al. (2020) Selenium, antioxidants, cardiovascular disease, and all-cause mortality: a systematic review and meta-analysis of randomized controlled trials. Am J Clin Nutr 112:1642-1652. https://pubmed.ncbi.nlm.nih.gov/33053149 53. Dziegielewska-Gesiak, S. (2021) Metabolic Syndrome in an Aging Society - Role of Oxidant-Antioxidant Imbalance and Inflammation Markers in Disentangling Atherosclerosis. Clin Interv Aging 16:1057-1070. https://pubmed.ncbi.nlm.nih.gov/34135578 54. Hajizadeh-Sharafabad F, Sharifi Zahabi, E. (2020) Role of alpha-lipoic acid in vascular function: A systematic review of human intervention studies. Crit Rev Food Sci Nutr 2020 Dec 17,1-14. https://pubmed.ncbi.nlm.nih.gov/33327738 55. Lederer AM, Fredriksen PM, Nkeh-Chungag BN, et al. (2021) Cardiovascular effects of air pollution: current evidence from animal and human studies. Am J Physiol Heart Circ Physiol 320:H1417-H1439. https://pubmed.ncbi.nlm.nih.gov/33513082 56. Fadaei R, Safari-Faramani R, Hosseini H, et al. (2021) Increased the circulating levels of malondialdehyde in patients with obstructive sleep apnea: a systematic review and meta-analysis. Sleep Breath 25:1753-1760. https://pubmed.ncbi.nlm.nih.gov/33560487 57. Hayes JD, Dinkova-Kostova AT, Tew KD (2020) Oxidative Stress in Cancer. Cancer Cell 38:167-197. https://pubmed.ncbi.nlm.nih.gov/32649885 58. Sosa V, Moliné T, Somoza R, et al. (2013) Oxidative stress and cancer: An overview. Ageing Research Reviews 12:376-390. https://pubmed.ncbi.nlm.nih.gov/23123177 59. Arfin S, Jha NK, Jha SK, et al. (2021) Oxidative Stress in Cancer Cell Metabolism. Antioxidants 10:642. https://pubmed.ncbi.nlm.nih.gov/33922139 60. Storz, P. Oxidative Stress in Cancer. In Oxidative Stress and Redox Regulation (eds. Jakob, U. & Reichmann, D.) pp427-447 (Springer Netherlands, 2013). http://doi.org/10.1007/978-94-007-5787-5_15. 61. Mas-Bargues C, Escrivá C, Dromant M, et al. (2021) Lipid peroxidation as measured by chromatographic determination of malondialdehyde. Human plasma reference values in health and disease. Arch Biochem Biophys 709:108941. https://pubmed.ncbi.nlm.nih.gov/34097903 62. Daiber A, Hahad O, Andreadou I, et al. (2021) Redox-related biomarkers in human cardiovascular disease - classical footprints and beyond. Redox Biol 42:101875. https://pubmed.ncbi.nlm.nih.gov/33541847 63. Chen X, Kang R, Kroemer G, Tang D (2021) Broadening horizons: the role of ferroptosis in cancer. Nat Rev Clin Oncol 18:280-296. https://pubmed.ncbi.nlm.nih.gov/33514910 64. Chang Y-T, Chang W-N, Tsai N-W, et al. (2014) The Roles of Biomarkers of Oxidative Stress and Antioxidant in Alzheimer's Disease: A Systematic Review. Biomed Res Int 2014:182303. https://pubmed.ncbi.nlm.nih.gov/24949424 65. Notarnicola M, Osella AR, Caruso MG, et al. (2021) Nonalcoholic Fatty Liver Disease: Focus on New Biomarkers and Lifestyle Interventions. Int J Mol Sci 22:3899. https://pubmed.ncbi.nlm.nih.gov/33918878 66. Gonzalo H, Brieva L, Tatzber F, et al. (2012) Lipidome analysis in multiple sclerosis reveals protein lipoxidative damage as a potential pathogenic mechanism. J Neurochem 123:622-634. https://pubmed.ncbi.nlm.nih.gov/22924648 67. Paliogiannis P, Fois AG, Sotgia S, et al. (2018) Circulating malondialdehyde concentrations in patients with stable chronic obstructive pulmonary disease: a systematic review and meta-analysis. Biomark Med 12:771-781. https://pubmed.ncbi.nlm.nih.gov/29865860 68. Kang Q, Yang C (2020) Oxidative stress and diabetic retinopathy: Molecular mechanisms, pathogenetic role and therapeutic implications. Redox Biol 37:101799. https://pubmed.ncbi.nlm.nih.gov/33248932 69. Cannavò SP, Riso G, Casciaro M, et al. (2019) Oxidative stress involvement in psoriasis: a systematic review. Free Radic Res 53:829-840. https://pubmed.ncbi.nlm.nih.gov/31392915 70. Noorimotlagh Z, Azizi M, Pan H-F, et al. (2020) Association between air pollution and Multiple Sclerosis: A systematic review. Environ Res 196:110386. https://pubmed.ncbi.nlm.nih.gov/33129851 71. Xie Z, Hou H, Luo D, et al. (2021) ROS-Dependent Lipid Peroxidation and Reliant Antioxidant Ferroptosis-Suppressor-Protein 1 in Rheumatoid Arthritis: a Covert Clue for Potential Therapy. Inflammation 44:35-47. https://pubmed.ncbi.nlm.nih.gov/32920707 72. Rodrigues P, Bochi GV, Trevisan G (2021) Advanced Oxidative Protein Products Role in Multiple Sclerosis: a Systematic Review and Meta-analysis. Mol Neurobiol 58:5724-5742. https://pubmed.ncbi.nlm.nih.gov/34392502 73. Jiang J, Chu C, Wu C, et al. (2021) Efficacy of probiotics in multiple sclerosis: a systematic review of preclinical trials and meta-analysis of randomized controlled trials. Food Funct 12:2354-2377. https://pubmed.ncbi.nlm.nih.gov/33629669 74. Kermani-Alghoraishi M, Pouramini A, Kafi F, Khosravi A (2021) Coronavirus Disease 2019 (COVID-19) and Severe Pericardial Effusion: From Pathogenesis to Management: A Case Report Based Systematic Review. Curr Probl Cardiol 47:100933. https://pubmed.ncbi.nlm.nih.gov/34404552 75. Wijeratne T, Gillard Crewther S, Sales C, Karimi L (2020) COVID-19 Pathophysiology Predicts That Ischemic Stroke Occurrence Is an Expectation, Not an Exception-A Systematic Review. Front Neurol 11:607221. https://pubmed.ncbi.nlm.nih.gov/33584506 76. Sengupta P, Leisegang K, Agarwal A (2021) The impact of COVID-19 on the male reproductive tract and fertility: A systematic review. Arab J Urol 19:423-436. https://pubmed.ncbi.nlm.nih.gov/34552795 77. Fakhrolmobasheri M, Mazaheri-Tehrani S, Kieliszek M, et al. (2021) COVID-19 and Selenium Deficiency: a Systematic Review. Biol Trace Elem Res. 2021 Nov 5;1-12 https://pubmed.ncbi.nlm.nih.gov/34739678 78. Skalny AV, Rossi Lima TR, Ke T, et al. (2020) Toxic metal exposure as a possible risk factor for COVID-19 and other respiratory infectious diseases. Food Chem Toxicol 146:111809. https://pubmed.ncbi.nlm.nih.gov/33069759 79. Ozdemir K (2021) Comparison of Oxidative Stress Parameters, Trace, Element and Quality of Life Levels in Healthy Women Before and After Covid-19 Vaccines. US Nat. Lib. Med. https://clinicaltrials.gov/ct2/show/NCT04751721. 80. Pierce JD, Shen Q, Cintron SA, Hiebert JB (2021) Post-COVID-19 Syndrome. Nurs Res. 2021 Oct 12; https://pubmed.ncbi.nlm.nih.gov/34653099 81. Mondelli V, Pariante CM (2021) What can neuroimmunology teach us about the symptoms of long-COVID? Oxf Open Immunol 2:iqab004. https://pubmed.ncbi.nlm.nih.gov/34192271 82. Cumpstey AF, Clark AD, Santolini J, et al. (2021) COVID-19: A Redox Disease-What a Stress Pandemic Can Teach Us About Resilience and What We May Learn from the Reactive Species Interactome About Its Treatment. Antioxid Redox Signal 35:1226-1268. https://pubmed.ncbi.nlm.nih.gov/33985343 83. Kalyanaraman, B. (2021) Reactive oxygen species, proinflammatory and immunosuppressive mediators induced in COVID-19: overlapping biology with cancer. RSC Chem Biol 2:1402-1414. https://pubmed.ncbi.nlm.nih.gov/34704045 84. Theoharides TC Conti P (2021) Be aware of SARS-CoV-2 spike protein: There is more than meets the eye. J Biol Regul Homeost Agents 35:833-838. https://pubmed.ncbi.nlm.nih.gov/34100279 85. DiNicolantonio JJ, O'Keefe JH (2018) Importance of maintaining a low omega-6/omega-3 ratio for reducing inflammation. Open Heart 5:e000946. https://pubmed.ncbi.nlm.nih.gov/30564378 86. Halliwell B, Gutteridge J (2015) Free radicals in biology and medicine. Oxford Univ Press, ISBN-13: 978-0198717485. https://usa1lib.org/book/2946453/86962c. 87. Mulkidjanian AY, Shalaeva DN, Lyamzaev KG, Chernyak BV (2018) Does Oxidation of Mitochondrial Cardiolipin Trigger a Chain of Antiapoptotic Reactions? Biochemistry (Mosc) 83:1263-1278. https://pubmed.ncbi.nlm.nih.gov/30472963 88. Seyfried TN, Arismendi-Morillo G, Mukherjee P, Chinopoulos C (2020) On the Origin of ATP Synthesis in Cancer. iScience 23:101761. https://pubmed.ncbi.nlm.nih.gov/33251492 89. Seyfried TN (2012) Cancer as a Metabolic Disease: On the Origin, Management, and Prevention of Cancer. Wiley, 2012. ISBN-13: 978-0470584927. 90. Seyfried, T. 癌症是一种代谢疾病:论癌症起源,治疗与预防。主译: 成长. (科学出版社, 2018). 91. Simopoulos AP (2002) The importance of the ratio of omega-6/omega-3 essential fatty acids. Biomed. Pharmacother. 56:365-379. https://pubmed.ncbi.nlm.nih.gov/12442909 92. Innes JK, Calder PC (2018) Omega-6 fatty acids and inflammation. Prostaglandins Leukot Essent Fatty Acids 132:41-48. https://pubmed.ncbi.nlm.nih.gov/29610056 93. Simopoulos AP (2016) An Increase in the Omega-6/Omega-3 Fatty Acid Ratio Increases the Risk for Obesity. Nutrients 8:128. https://pubmed.ncbi.nlm.nih.gov/26950145 94. Simopoulos AP (2008) The importance of the omega-6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med (Maywood) 233:674-688. https://pubmed.ncbi.nlm.nih.gov/18408140 95. Guyenet SJ, Carlson SE (2015) Increase in adipose tissue linoleic acid of US adults in the last half century. Adv Nutr 6:660-664. https://pubmed.ncbi.nlm.nih.gov/26567191 96. Huang H-Y, Appel LJ, Croft KD, et al. (2002) Effects of vitamin C and vitamin E on in vivo lipid peroxidation: results of a randomized controlled trial. Am J Clin Nutr. 76:549-555. https://pubmed.ncbi.nlm.nih.gov/12197998 97. Cadenas E, Sies H (1998) The lag phase. Free Radic Res 28:601-609. https://pubmed.ncbi.nlm.nih.gov/9736312 98. Barclay LR (1988) The cooperative antioxidant role of glutathione with a lipid-soluble and a water-soluble antioxidant during peroxidation of liposomes initiated in the aqueous phase and in the lipid phase. J Biol Chem 263:16138-16142. https://pubmed.ncbi.nlm.nih.gov/3182788 99. Reider CA, Chung RY, Devarshi PP, et al. (2020) Inadequacy of Immune Health Nutrients: Intakes in US Adults, the 2005-2016 NHANES. Nutrients 12:1735. https://pubmed.ncbi.nlm.nih.gov/32531972 100. Rasmussen, M. (2020) Vitamin C Evidence for Treating Complications of COVID-19 and other Viral Infections. Orthomolecular Medicine News Service. http://orthomolecular.org/resources/omns/v16n25.shtml 101. Levy TE (2021) Rapid Virus Recovery. Medfox Pub. ISBN-13: 978-0998312415. https://rvr.medfoxpub.com 102. Levy TE (2021) Hydrogen Peroxide Nebulization and COVID Resolution. Orthomolecular Medicine News Service. http://orthomolecular.org/resources/omns/v17n13.shtml 103. Caruso AA, Del Prete A, Lazzarino AI (2020) Hydrogen peroxide and viral infections: A literature review with research hypothesis definition in relation to the current covid-19 pandemic. Med Hypotheses 144:109910. https://pubmed.ncbi.nlm.nih.gov/32505069 104. Cervantes Trejo, A, Castañeda ID, Cortés Rodríguez A, et al. (2021) Hydrogen Peroxide as an Adjuvant Therapy for COVID-19: A Case Series of Patients and Caregivers in the Mexico City Metropolitan Area. Evid Based Complement Alternat Med. 2021:5592042. https://pubmed.ncbi.nlm.nih.gov/34335827 105. Nathan CF, Cohn ZA (1981) Antitumor effects of hydrogen peroxide in vivo. J Exp Med 154:1539-1553. https://pubmed.ncbi.nlm.nih.gov/7299347 106. Finney JW, Urschel HC, Balla GA, et al. (1967) Protection of the ischemic heart with DMSO alone or DMSO with hydrogen peroxide. Ann N Y Acad Sci 141:231-241. https://pubmed.ncbi.nlm.nih.gov/5232232 107. Levy TE (2021) Vitamin C and Cortisol: Synergistic Infection and Toxin Defense. Orthomolecular Medicine News Service. http://orthomolecular.org/resources/omns/v17n28.shtml Nutritional Medicine is Orthomolecular MedicineOrthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org Find a DoctorTo locate an orthomolecular physician near you: http://orthomolecular.org/resources/omns/v06n09.shtml The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource. Editorial Review Board:
Albert G. B. Amoa, MB.Ch.B, Ph.D. (Ghana)
Comments and media contact: editor@orthomolecular.org OMNS welcomes but is unable to respond to individual reader emails. Reader comments become the property of OMNS and may or may not be used for publication. To Subscribe at no charge: http://www.orthomolecular.org/subscribe.html To Unsubscribe from this list: http://www.orthomolecular.org/unsubscribe.html |

This website is managed by Riordan Clinic
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2017
Consult your orthomolecular health care professional for individual guidance on specific health problems.