|

|
|
|
|
|
This article may be reprinted free of charge provided 1) that there is clear attribution to the Orthomolecular Medicine News Service, and 2) that both the OMNS free subscription link http://orthomolecular.org/subscribe.html and also the OMNS archive link http://orthomolecular.org/resources/omns/index.shtml are included. FOR IMMEDIATE RELEASE
Summary of Recent Research with Three Nutrients in the War Against Cancer
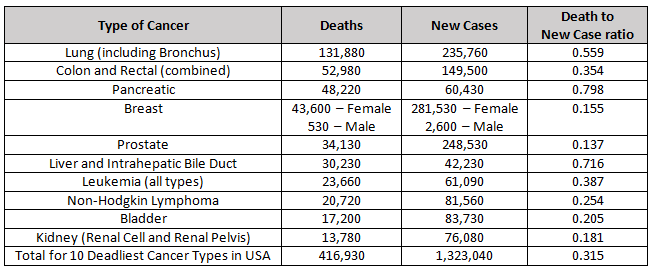
by Michael PasswaterOMNS (Nov. 11, 2021) We have much to learn about preventing and treating cancer. Each disease in the cohort of cancers is potentially a different disease related to the specific genetic mutations that drive it. In the interest of promoting further efforts to improve our understanding of these complex diseases, here is an update on research involving three essential nutrients: vitamin C, selenium (selenite and methyl selenocysteine), and vitamin E (delta tocotrienol). Although much progress has been made in the fight against some types of cancer, many types still remain literally a death sentence. Each year, more than 1.3 million people are diagnosed with one of the ten most deadly types of cancer in the United States and over 400,000 people die from these dreaded diseases. 2021 Estimated Cancer Deaths and New Cases in the United States [1]
Ascorbic Acid (Vitamin C)By definition, a vitamin is essential for life, and vitamin C (ascorbic acid) is no exception. The health benefits of vitamin C are so extensive that it would be an important tool in the battle against cancer even without its powerful anti-tumor effect. Vitamin C is important for many aspects of immune and endothelial health; synthesis of catecholamines, carnitine, neuropeptides, neurotransmitters, collagen, and elastin; breakdown of L-tyrosine and hypoxic inducible factor 1-alpha (HIF-1a); epigenomic regulation; somatic stem cell reprogramming; and redox regulation including scavenging damaging free radicals, breaking chains of lipid peroxidation, and recycling other antioxidants. [2-8] In 1976, Cameron and Pauling reported longer survival in terminal cancer patients given vitamin C. [9] Was this from improvement to the patients' constitution, was there an anti-tumor effect, or both? We now know that high doses of vitamin C can have a prooxidant effect, especially in combination with iron, which can selectively kill tumor cells containing less catalase than healthy human cells. [10, 11] The catalase enzyme is necessary for nearly all cells to remove hydrogen peroxide that can cause free radicals and damage the cell's biomolecules, including proteins and DNA. And vitamin C can also disrupt the "Warburg Effect" in tumor cells. [12,13,14] The Warburg Effect is the tendency of tumor cells to switch from using mitochondrial oxidative phosphorylation to aerobic glycolysis for the production of cellular energy (ATP). While greatly reducing the efficiency of energy production (2 ATP molecules generated per glucose molecule vs. 36 ATP molecules generated per glucose molecule), aerobic glycolysis enhances the ability of the cell to proliferate. Efficiency is only important when resources are scarce. In a glucose rich environment, 2 ATP molecules per glucose will work just fine, and allows more of the glucose, along with the amino acid glutamine, to provide the structures necessary to make additional tumor cells. This primitive, yet streamlined, tumor metabolism allows abundantly available glucose and glutamine to supply the biochemical needs of cell growth and division. Many tumor cells over-express glucose transporters, particularly GLUT1 to increase intake of glucose. Ascorbic acid, and especially oxidized ascorbic acid (dehydroascorbic acid) is similar in molecular shape to glucose, and can enter cells through these membrane transport channels. Not only does this disrupt the supply of glucose to the tumor cell, it also allows increased vitamin C concentrations within the cell where it can cause epigenetic effects including increasing TET enzyme activity, re-expression of tumor suppressor genes, or cause cell death through metabolic disruption. Depletion of intracellular glutathione leads to inactivation of glyceraldehyde 3-phosphate dehydrogenase and inhibition of glycolysis. In the setting of high vitamin C concentrations, the reliance of some tumor cells on aerobic glycolysis becomes their "Achilles' heel". [15] In recent years, cell culture studies and human clinical trials have confirmed that tumor cells with KRAS and BRAF mutations can be selectively killed by appropriate doses of vitamin C. [16] KRAS and BRAF mutations are common in solid tumors, especially pancreatic, colon, and lung cancers. Synergistic effects have been seen by combining vitamin C with some chemotherapy drugs, radiation treatment, or in combination with a fasting-mimicking diet. [17-23] Mark Levine, Channing Paller, Tami Tamashiro, Thomas Luechtefeld and Amy Gravell recently reviewed 53 cancer clinical trials involving IV and/or oral vitamin C. [15] These trials give a clear signal of safety when patients with glucose 6 phosphate dehydrogenase (G6PD) deficiency are excluded from high dose IVC administration. Most studies were small, and involved a wide variety of late stage cancers. Nonetheless, encouraging signals were seen, including a few patients surviving years later eventually dying of causes other than cancer. Studies involving pancreatic ductal adenocarcinoma (PDAC) show a median survival following diagnosis of 3.5 months untreated, 6.7 months when treated with gemcitabine, 8.5 - 13 months when treated with gemcitabine and nab-paclitaxel, and 15.1 months when IVC with or without gemcitabine was used. [17,24] It is likely that with refinement of dosing and route of administration, earlier intervention, and improved knowledge of which tumors are most susceptible to high dose vitamin C therapy, more consistent positive results will be seen. Three promising active clinical trials: A Phase II Trial of Pharmacological Ascorbate, Gemcitabine, and Nab-Paclitaxel for Metastatic Pancreatic Cancer (PACMAN 2.1; University of Iowa Holden Comprehensive Cancer Center) [25] A Phase II Study of High Dose Vitamin C Intravenous Infusion in Patients with Resectable or Metastatic Solid Tumor Malignancies (Weill Cornell Medicine, NYC) [26] To download an informative description of "IV Vitamin C for Cancer Care", please click
https://riordanclinic.org/wp-content/uploads/2017/09/IVChandout.pdf. SeleniumSelenium is a micronutrient essential for human health. There are 25 human selenoproteins known to be involved in numerous functions throughout the body, including brain, blood vessel, heart, and immune system health. These proteins perform diverse functions including antioxidant and redox recycling, gene "proof-reading", vitamin D metabolism, and hemostasis. Like vitamin C, even if there were no direct tumor effect of selenium, it would be an important tool in the battle for wellness and against cancer. [28-31] HLA-E is a "camouflage protein" expressed by some tumors to hide from the immune system. The protein fools the immune system into thinking the tumor cell is a normal cell. A decade ago, selenite was shown to reduce - nearly eliminate - HLA-E expression on tumor cells. The tumor cells then became susceptible to destruction by Natural Killer cells (immune cells which clear unhealthy cells from the body). [32] A recent study of 243 PDAC patients showed that higher HLA-E and HLA-G (a similar protein) expression was associated with shorter survival. [33] In addition to optimizing tissue health throughout the body, the reduction of camouflage membrane proteins HLA-E and HLA-G by selenite may be a useful tool in the battle against cancer. Of note, selenomethionine (SeMet) had no effect on tumor cell HLA-E expression. Selenomethionine was the form of selenium used in the SELECT trial which did not show a benefit of selenium against prostate cancer prevention. In addition to the unfortunate choice of selenium supplement, the trial had other flaws, including a lack of difference in selenium levels between the control and test groups. Methyl selenocysteine (MSC) was the form of selenium used in the Nutritional Prevention of Cancer (NPC) trial which showed benefit. MSC is also the dominant form of selenium in broccoli, cabbage, onions and garlic. In 2014, MSC was shown to protect against the toxicity of four chemotherapy agents (cyclophosphamide, cisplatin, oxalplatin, and irinotecan), and enhance antitumor activity. [34] More recently, a phase I study at Stanford using selenite and radiation therapy in humans validated the further study of selenite against cancer. [35] Additionally, in vitro and in vivo (mice) studies at the University of Grenada showed a strong antitumor effect of selenite against pancreatic cancer, alone and in combination with gemcitabine. [36] Delta TocotrienolVitamin E is an essential nutrient for humans. Vitamin E is a lipid soluble antioxidant. There are 8 different molecules in the vitamin E family pertinent to humans. It comprises 4 tocopherols (alpha, beta, gamma, delta), and 4 tocotreinols (alpha, beta, gamma, delta). Tocotreinols are smaller than tocopherols and are unsaturated. Tocotrienols have a half-life of approximately 4 hours while tocopherols have a half-life of 20 hours. Delta tocotrienol (VEDT = Vitamin E Delta Tocotrienol) is the smallest member of the vitamin E family, as it has the shortest "tail". Its small size allows delta tocotrienol greater mobility within lipid layers of cell membranes. Studies have shown that tocotreinols inhibit Nuclear factor kappa B (NF-kB) activity and human pancreatic cancer cell survival, with VEDT having the strongest effect. [37] NF-kB is involved in immune and inflammatory responses, and in the regulation of cellular gene expression, proliferation, differentiation, and survival. VEDT has also been shown to enhance gemcitabine activity in pancreatic cancer cells. [38-40] Furthermore, VEDT has been shown to inhibit PDAC stem-like cells. VEDT significantly inhibited growth and metastases of these cells, including inhibiting the growth and metastasis of gemcitabine resistant PDAC stem-cell-like cells. [41] A phase I human clinical trial at Moffitt Cancer Center in Tampa, Florida showed 200 to 1600 mg VEDT taken orally daily for 2 weeks was well tolerated and significantly induced apoptosis (cell death) in pancreatic ductal cancer cells. [42] An anti-tumor effect, as well as a reduction in side effects from chemotherapy, has also been shown in the setting of other solid tumors. [43-56] Note that to prevent the larger tocopherols from blocking absorption of the smaller tocotreinols, it is best to avoid taking tocopherols at the same time as tocotrienols. [57-63] Twice daily dosing of tocotrienols have been shown to produce a steady state after three days. SummaryThe redox synergy of vitamin C, vitamin E, and selenium-containing glutathione peroxidases has been explored since the 1960s and 1970s. Studies focusing on single nutrient interventions, with and without chemotherapy and radiation, have suggested benefit in humans, with increasingly specific mechanistic and treatment details discovered each decade. Along the way, a reassuring safety profile of nutrient interventions with and without traditional chemotherapy and radiation interventions has been established. Further studies to better define the most effective match of treatment for each tumor type, along with the best route, dose, and combination of treatments are important next steps to improve the reliability and effectiveness of preventing and treating the many types of cancer. Combining nutrients known to be synergistic together, while limiting glucose and glutamine central to the metabolism of many tumor cells, may optimize the effectiveness of treatment strategies. With nutrient therapy - orthomolecular medicine - one does not need to choose between attacking the tumor and strengthening the host. The treatments often impact both simultaneously. Foundational Support
Advanced Support
(Michael Passwater is certified by the American Society for Clinical Pathology as a Medical Technologist, a specialist in Immunohematology, and a diplomate in Laboratory Management. He has worked in clinical laboratories for 28 years, and has his degree in Medical Technology from the University of Delaware.) References & Further Reading1. National Cancer Institute. Common Cancer Types. https://www.cancer.gov/types/common-cancers 2. Oudemans-van Straaten HM, Spoelstra-de Man AME, de Waard MC. (2014) Vitamin C revisited. Critical Care 18:460-473. https://pubmed.ncbi.nlm.nih.gov/25185110 3. Manning J, Mitchell B, Appaduras DA, May JM, et al. (2013) Vitamin C Promotes Maturation of T-Cells. Antioxid Redox Signal. 19:2054-2067. https://pubmed.ncbi.nlm.nih.gov/23249337 4. Ladumer A, Schmitt CA, Schachner D, et al. (2012) Ascorbate stimulates endothelial nitric oxide synthase enzyme activity by rapid modulation of its phosphorylation status. Free Radic Biol Med. 2012 May 15; 52:2082-2090. https://pubmed.ncbi.nlm.nih.gov/22542797 5. May JM, Qu ZC. (2010) Ascorbic Acid Prevents Increased Endothelial Permeability Caused by Oxidized Low Density Lipoprotein. Free Radical Res. 44:1359-1368. https://pubmed.ncbi.nlm.nih.gov/20815791 6. Deicher R, Ziai F, Begknayer C, et al. (2005) Low Total Vitamin C Plasma Level Is a Risk Factor for Cardiovascular Morbidity and Mortality in Hemodialysis Patients. J Am Soc Nephrol. 16:1811-1818. https://pubmed.ncbi.nlm.nih.gov/15814831 7. Heller R, Munscher-Paulig F, Grabner R, Till V. (1999) L-Ascorbic Acid Potentiates Nitric Oxide Synthesis in Endothelial Cells. J Biol Chem, 274:8254-8260. https://pubmed.ncbi.nlm.nih.gov/10075731 8. Leibovitz B, Siegel BV. (1978) Ascorbic acid, neutrophil function, and the immune response. Int J Vitam Nutr Res. 48:159-164. https://pubmed.ncbi.nlm.nih.gov/357320 9. Cameron E, Pauling L. (1976) Supplemental ascorbate in the supportive treatment of cancer: Prolongation of survival times in terminal human cancer. Proc Natl Acad Sci USA. 73: 3685-3689. https://pubmed.ncbi.nlm.nih.gov/1068480 10. Schoenfeld JD, Sibenaller ZA Mapuskar KA, et al (2017) O2- and H2O2-Mediated Disruption of Fe Metabolism Causes the Differential Susceptibility of NSCLC and GBM Cancer Cells to Pharmacological Ascorbate. Cancer Cell 31: 487-500. https://pubmed.ncbi.nlm.nih.gov/28366679 11. O'Leary BR, Alexander MS, Du J, et al (2020) Pharmacological ascorbate inhibits pancreatic cancer metastases via a peroxide-mediated mechanism. Sci Rep 10:17649 https://pubmed.ncbi.nlm.nih.gov/33077776. 12. Aguilera O, Muñoz-Sagastibelza M, Torrejón E, et al. (2016) Vitamin C uncouples the Warburg metabolic switch in KRAS mutant colon cancer. Oncotarget, 7:47954-47965. https://pubmed.ncbi.nlm.nih.gov/27323830 13. Suzuki T, Kishikawa T, Sato T, et al. (2021) Mutant KRAS drives metabolic reprogramming and autophagic flux in premalignant pancreatic cells. Cancer Gene Ther. Online ahead of print. https://pubmed.ncbi.nlm.nih.gov/33833413 14. Gonzalez MJ, Seyfried T; Nicolson GL et al. (2018) Mitochondrial Correction: A New Therapeutic Paradigm for Cancer and Degenerative Diseases. J Orthomolecular Med 33: 4. https://riordanclinic.org/journal-article-archive/mitochondrial-correction-a-new-therapeutic-paradigm-for-cancer-and-degenerative-diseases 15. Chen Q, Vissers MCM (2020) Cancer and Vitamin C. CRC Press. ISBN-13: 978-0367858049 16. Yun J, Mullarky E, Lu C, et al. (2015) Vitamin C selectively kills KRAS and BRAF mutant colorectal cancer cells by targeting GAPDH. Science 350:1391-1396. https://pubmed.ncbi.nlm.nih.gov/26541605 17. Polireddy K, Dong R, Reed G, et al. (2017) High Dose Parenteral Ascorbate Inhibited Pancreatic Cancer Growth and Metastasis: Mechanisms and a Phase I/IIa study. Sci Rep 7: 17188 https://pubmed.ncbi.nlm.nih.gov/29215048 18. Alexander MS, Wilkes JG, Schroeder SR, Buettner GR. (2018) Pharmacologic ascorbate reduces radiation-induced normal tissue toxicity and enhances tumor radiosensitization in pancreatic cancer. Cancer Res. 78:6838-6851. https://pubmed.ncbi.nlm.nih.gov/30254147. 19. Drisko JA, Serrano OK, Spruce LR, Chen Q, Levine M. (2018) Treatment of pancreatic cancer with intravenous vitamin C: a case report. Anti-Cancer Drugs 29:373-379. https://pubmed.ncbi.nlm.nih.gov/29438178 20. Welsh JL, Wagner BA, van't Erve TJ, et al. (2013) Pharmacological ascorbate with gemcitabine for the control of metastatic and node-positive pancreatic cancer (PACMAN): results from a phase I clinical trial. Cancer Chemother. Pharmacol. 71:765-775. https://pubmed.ncbi.nlm.nih.gov/23381814 21. Monti DA, Mitchell E, Bazzan AJ, et al. (2012) Phase I evaluation of intravenous ascorbic acid in combination with gemcitabine and erlotinib in patients with metastatic pancreatic cancer. PLoS ONE 7(1):e29794. https://pubmed.ncbi.nlm.nih.gov/22272248 22. Mikirova N, Casciari J, Hunninghake R. (2019) Continuous Intravenous Vitamin C in the Cancer Treatment: Reevaluation of a Phase I Clinical Study. Functional Foods in Health and Disease. https://riordanclinic.org/journal-article-archive/continuous-intravenous-vitamin-c-in-the-cancer-treatment-reevaluation-of-a-phase-i-clinical-study 23. Di Tano M, Raucci F, Vernieri C, et al. (2020) Synergistic effect of fasting-mimicking diet and vitamin C against KRAS mutated cancers. Nat Comm 11:2332 https://pubmed.ncbi.nlm.nih.gov/32393788 24. Carr AC, Cook J. (2018) Intravenous Vitamin C for Cancer Therapy -- Identifying the Current Gaps in Our Knowledge. Front. Physiol. 9:1182. https://pubmed.ncbi.nlm.nih.gov/30190680 25. Cullen JJ (2021) A Phase II Trial of Pharmacological Ascorbate, Gemcitabine, and Nab-Paclitaxel for Metastatic Pancreatic Cancer (PACMAN 2.1) https://clinicaltrials.gov/ct2/show/NCT02905578 26. Shah MA, Khan U. (2021) A Phase II Study of High Dose Vitamin C Intravenous Infusion in Patients with Resectable or Metastatic Solid Tumor Malignancies. https://jcto.weill.cornell.edu/open_clinical_trials/a-phase-ii-study-of-high-dose-vitamin-c-intravenous-infusion-in-patients-with-resectable-or-metastatic-solid-tumor-malignancies 27. Riordan Clinic (2021) High Dose IV Vitamin C (IVC) https://riordanclinic.org/what-we-do/high-dose-iv-vitamin-c 28. Grimble RF. (2001) Nutritional modulation of immune function. Proc. Nutr. Soc. 60:389-397. https://pubmed.ncbi.nlm.nih.gov/11681814 29. Arthur JR, McKenzie RC, Beckett GJ. (2003) Selenium in the immune system. J. Nutr. 133:1457S-1459S. https://pubmed.ncbi.nlm.nih.gov/12730442 30. Guillin OM, Vindry C, Ohlmann T, Chavatte L. (2019) Selenium, Selenoproteins, and Viral Infection. Nutrients, 11:2101. https://pubmed.ncbi.nlm.nih.gov/31487871 31. Huang Z, Rose AH, Hoffman PR. (2012) The Role of Selenium in Inflammation and Immunity: From Molecular Mechanisms to Therapeutic Opportunities. Antioxid Redox Signal. 16:705-743. https://pubmed.ncbi.nlm.nih.gov/21955027 32. Enqvist M, Nilsonne G, Hammarfjord O, et al, (2011) Selenite Induces Posttranscriptional Blockade of HLA-E Expression and Sensitizes Tumor Cells to CD94/NKG2A-Positive NK Cells. J Immunol. 187:3546-3554. https://pubmed.ncbi.nlm.nih.gov/21890659 33. Hiraoka N, Ino Y, Hori S, et al. (2020) Expression of classical human leukocyte antigen class I antigens, HLA-E and HLA-G, is adversely prognostic in pancreatic cancer patients Cancer Sci. 111:3057-3070. https://pubmed.ncbi.nlm.nih.gov/32495519 34. Cao S, Durrani FA, Tóth K, Rustum YM. (2014) Se-methylselenocysteine offers selective protection against toxicity and potentiates the antitumour activity of anticancer drugs in preclinical animal models Br J Cancer 110:1733-1743. https://pubmed.ncbi.nlm.nih.gov/24619073 35. Knox SJ, Jayachandran P, Keeling CA, et al. (2019) Results from a Phase 1 Study of Sodium Selenite in Combination with Palliative Radiation Therapy in Patients with Metastatic Cancer. Transl Oncol. 12:1525-1531. https://pubmed.ncbi.nlm.nih.gov/31454725 36. Doello K, Mesas C, Quiñonero F, et al. (2021) The Antitumor Activity of Sodium Selenite Alone and in Combination with Gemcitabine in Pancreatic Cancer: An In Vitro and In Vivo Study. Cancers. 13:3169. https://pubmed.ncbi.nlm.nih.gov/34201986 37. Husain K, Francois RA, Yamauchi T, et al. (2011) Vitamin E delta-tocotrienol augments the antitumor activity of gemcitabine and suppresses constitutive NF-kappaB activation in pancreatic cancer. Mol Cancer Ther. 10:2363-2372. https://pubmed.ncbi.nlm.nih.gov/21971120 38. Malafa MP, Sebti S, (2014) Delta-Tocotrienol Treatment and Prevention of Pancreatic Cancer. Lee Moffitt Cancer Center & Research Institute, University of South Florida (Tampa): US Patent US 8,846,653. https://patentimages.storage.googleapis.com/c7/ff/ef/b836e04b18be57/US8846653.pdf 39. Hussein D, Mo H. (2009) d-Delta-tocotrienol-mediated suppression of the proliferation of human PANC-1, MIA PaCa-2, and BxPC-3 pancreatic carcinoma cells. Pancreas. 38:e124-e136. https://pubmed.ncbi.nlm.nih.gov/19346993 40. Husain K, Centeno BA, Chen D-T, et al. (2013) Vitamin E delta-tocotrienol prolongs survival in the LSLKrasG12D/+;LSL-Trp53R172H/+;Pdx-1-Cre (KPC) transgenic mouse model of pancreatic cancer. Cancer Prev Res (Phila). 6:1074-83. https://pubmed.ncbi.nlm.nih.gov/23963802 41. Husain K, Centeno BA, Coppola D, et al. (2017) d-Tocotrienol, a natural form of vitamin E, inhibits pancreatic cancer stem-like cells and prevents pancreatic cancer metastasis. Oncotarget. 8:31554-31567. https://pubmed.ncbi.nlm.nih.gov/28404939 42. Springett GM, Husain K, Neuger A, et al. (2015) A Phase I Safety, Pharmacokinetic, and Pharmacodynamic Presurgical Trial of Vitamin E d-tocotrienol in Patients with Pancreatic Ductal Neoplasia EBioMedicine 2:1987-1995. https://pubmed.ncbi.nlm.nih.gov/26844278 43. Guthrie N, Gapor A, Chambers AF, Carroll KK. (1997) Inhibition of proliferation of estrogen receptor-negative MDA-MB-435 and -positive MCF-7 human breast cancer cells by palm oil tocotrienols and tamoxifen, alone and in combination. J Nutr. 127:544S-548S. https://pubmed.ncbi.nlm.nih.gov/9082043 44. Nesaretnam K, Stephen R, Dils R, Darbre P. (1998) Tocotrienols inhibit the growth of human breast cancer cells irrespective of estrogen receptor status. Lipids. 33:461-469. https://pubmed.ncbi.nlm.nih.gov/9625593 45. Shun M-C, Yu W, Gapor A, et al. (2004) Pro-apoptotic mechanisms of action of a novel vitamin E analog (alpha-TEA) and a naturally occurring form of vitamin E (delta-tocotrienol) in MDA-MB-435 human breast cancer cells. Nutr Cancer. 48:95-105. https://pubmed.ncbi.nlm.nih.gov/15203383 46. Kaneko S, Sato C, Shiozawa N, et al. (2018) Suppressive Effect of Delta-Tocotrienol on Hypoxia Adaptation of Prostate Cancer Stem-like Cells. Anticancer Res. 38:1391-1399. https://pubmed.ncbi.nlm.nih.gov/15203383 47. Ji X, Wang Z, Geamanu A, et al. (2012) Delta-tocotrienol suppresses Notch-1 pathway by upregulating miR-34a in nonsmall cell lung cancer cells. Int J Cancer. 131: 2668-2677. https://pubmed.ncbi.nlm.nih.gov/22438124 48. Ji X, Wang Z, Sarkar FH, Gupta SV. (2012) Delta-tocotrienol augments cisplatin-induced suppression of non-small cell lung cancer cells via inhibition of the Notch-1 pathway. Anticancer Res. 32:2647-2655. https://pubmed.ncbi.nlm.nih.gov/22753722 49. Nasr M, Nafee N, Saad H, Kazem A. (2014) Improved antitumor activity and reduced cardiotoxicity of epirubicin using hepatocyte-targeted nanoparticles combined with tocotrienols against hepatocellular carcinoma in mice. Eur J Pharm Biopharm. 88:216-225. https://pubmed.ncbi.nlm.nih.gov/24813390 50. Wada S, Naito Y, Matsushita Y, et al. (2017) Delta-tocotrienol suppresses tumorigenesis by inducing apoptosis and blocking the COX-2/PGE2 pathway that stimulates tumor-stromal interactions in colon cancer. J Funct Foods. 35:428-435. https://www.sciencedirect.com/science/article/pii/S1756464617303183 51. Shibata A, Nakagawa K, Tsuduki T, Miyazawa T. (2015) Delta-Tocotrienol treatment is more effective against hypoxic tumor cells than normoxic cells: potential implications for cancer therapy. J Nutr Biochem. 26:832-840. https://pubmed.ncbi.nlm.nih.gov/25979648 52. Zhang J-S, Li D-M, He N, et al. (2011) A paraptosis-like cell death induced by delta-tocotrienol in human colon carcinoma SW620 cells is associated with the suppression of the Wnt signaling pathway. Toxicology. 285:8-17. https://pubmed.ncbi.nlm.nih.gov/21453743 53. Sun W, Wang Q, Chen B, et al. (2008) Gamma-tocotrienol-induced apoptosis in human gastric cancer SGC-7901 cells is associated with a suppression in mitogen-activated protein kinase signalling. Br J Nutr. 99:1247-1254. https://pubmed.ncbi.nlm.nih.gov/18081943 54. Sun W, Xu W, Liu H, et al. (2009) gamma-Tocotrienol induces mitochondria-mediated apoptosis in human gastric adenocarcinoma SGC-7901 cells. J Nutr Biochem. 20:276-284. https://pubmed.ncbi.nlm.nih.gov/18602811 55. Satyamitra MM, Kulkarni S, Ghosh SP, et al. (2011) Hematopoietic Recovery and Amelioration of Radiation-Induced Lethality by the Vitamin E Isoform delta-Tocotrienol. Radiat Res. 175:736-745. https://pubmed.ncbi.nlm.nih.gov/21434782 56. Constantinou C, Charalambous C, Kanakis D. (2020) Vitamin E and cancer: an update on the emerging role of gamma and delta tocotrienols. Eur J Nutr. 59:845-857. https://pubmed.ncbi.nlm.nih.gov/31016386 57. Drotleff AM, Bohnsack C, Schneider I, et al. (2014) Human oral bioavailability and pharmacokinetics of tocotrienols from tocotrienol-rich (tocopherol-low) barley oil and palm oil formulations. J Funct Foods. 7:150-160. https://www.sciencedirect.com/science/article/pii/S1756464614000024 58. Szewczyk K, Chojnacka A, Górnicka M. (2021) Tocopherols and Tocotrienols -- Bioactive Dietary Compounds; What Is Certain, What Is Doubt? Int J Mol Sci. 22:6222. https://pubmed.ncbi.nlm.nih.gov/34207571 59. Trias AM, Tan B. (2013) Alpha-tocopherol: a detriment to tocotrienol benefits. In: Tan B, Watson RR, Preedy VR, eds. Tocotrienols: Vitamin E Beyond Tocopherols. 2nd ed. Boca Raton, FL: CRC Press; 2013. pp 61-78. ISBN-13: 978-1138199729 60. Qureshi AA, Pearce BC, Nor RM, et al. (1996) Dietary alpha-tocopherol attenuates the impact of gamma-tocotrienol on hepatic 3-hydroxy-3-methylglutaryl coenzyme A reductase activity in chickens. J Nutr. 126:389-394. https://pubmed.ncbi.nlm.nih.gov/8632210 61. Shibata A, Kawakami Y, Kimura T, et al. (2016) Alpha-tocopherol attenuates the triglyceride- and cholesterol-lowering effects of rice bran tocotrienol in rats fed a Western diet. J Agric Food Chem. 64:5361-5366. https://pubmed.ncbi.nlm.nih.gov/27295311 62. Shibata A, Nakagawa K, Tsuduki T, Miyazawa T. (2015) Alpha-tocopherol suppresses antiangiogenic effect of delta-tocotrienol in human umbilical vein endothelial cells. J Nutr Biochem, 26:345-50. https://pubmed.ncbi.nlm.nih.gov/25662730 63. Passwater R (2019) More Than Vitamin E: The Story & Science Behind Tocotrienols. Whole Foods Magazine. https://wholefoodsmagazine.com/columns/vitamin-connection/more-than-vitamin-e-the-story-science-behind-tocotrienols-part-1-tocotrienols-no-longer-the-obscure-member-of-the-vitamin-e-family 64. Penberthy WT, Saul AW, Smith RG, (2021) Niacin and Cancer How vitamin B-3 protects and even helps repair your DNA. Orthomolecular Medicine News Service. http://orthomolecular.org/resources/omns/v17n05.shtml 65. Diener E,Chan MY. (2011) Happy People Live Longer: Subjective Well-Being Contributes to Health and Longevity. Applied Psychology: Health and Well-Being. 3:1-43. https://doi.org/10.1111/j.1758-0854.2010.01045.x 66. Yuen RCF (2021) High Dose Vitamin C for Cancer: The Struggle with "Non-Evidence-Based" Medical Practice. Orthomolecular Medicine News Service, http://orthomolecular.org/resources/omns/v17n20.shtml Nutritional Medicine is Orthomolecular MedicineOrthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org Find a DoctorTo locate an orthomolecular physician near you: http://orthomolecular.org/resources/omns/v06n09.shtml The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource. Editorial Review Board:
Albert G. B. Amoa, MB.Ch.B, Ph.D. (Ghana)
Comments and media contact: editor@orthomolecular.org OMNS welcomes but is unable to respond to individual reader emails. Reader comments become the property of OMNS and may or may not be used for publication. To Subscribe at no charge: http://www.orthomolecular.org/subscribe.html To Unsubscribe from this list: http://www.orthomolecular.org/unsubscribe.html |

This website is managed by Riordan Clinic
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2017
Consult your orthomolecular health care professional for individual guidance on specific health problems.