|

|
|
|
|
|
This article may be reprinted free of charge provided 1) that there is clear attribution to the Orthomolecular Medicine News Service, and 2) that both the OMNS free subscription link http://orthomolecular.org/subscribe.html and also the OMNS archive link http://orthomolecular.org/resources/omns/index.shtml are included. FOR IMMEDIATE RELEASE
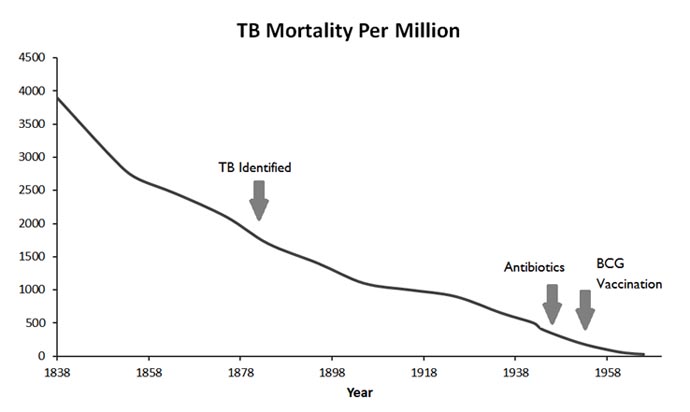
Progress with TB or a Return to the Dark Ages?by Steve Hickey, PhD and William B. Grant, PhD(OMNS June 17, 2013) Tuberculosis (TB) was formerly one of the most devastating scourges of mankind and remains a leading cause of death. The disease has been with humans over recorded history, and likely throughout the evolution of our species. Through the industrial revolution and into the 20 century, TB became a long term medical emergency particularly with the poor. Roughly one person in four was dying of the disease in England and similar death rates were observed in other modernising countries. One solution was to isolate the afflicted in sanatoria. The fresh air and sunlight solution practiced in those times may have been at least partly effective. Sunlight and vitamin D played an early role in preventing and treating TB. In the early 20th century, TB patients were often sent to sanatoria in the mountains where they were exposed to solar radiation. Dr. Auguste Rollier set up such facilities in the Swiss Alps. [1] Sun exposure is associated with a lower incidence of TB six months later. [2]. It wasn't until 2006-7 that researchers at UCLA determined how sunlight increased vitamin D levels and helps the body's immune system prevent bacterial infections [3]. Higher blood levels of 25-hydroxyvitamin D can reduce the time required to control TB during treatment. [4,5] Recent research suggests the sanatoria approach to treatment could have been at least partly effective. The modern myth about conquering infectious diseases such as TB is that vaccination and antibiotics came to the rescue, saving humanity from the earlier suffering. However, TB like the other major life threatening infections had already declined to a low level before these interventions were introduced. The tubercle bacillus was identified by Robert Koch in 1882 [6] by which time the death rates in England and Wales had already reduced to about half the earlier levels. The introduction of the drug isoniazid in the early 1950s was a breakthrough in antibiotic treatment but had little effect on overall mortality. Similarly, BCG vaccination was first tried in people in the early 1920s but its widespread introduction was delayed until well after World War 2. A chart of mortality from TB shows its historical decline in England and Wales for which the most extensive historical statistics are available. [7] The decline of TB was similar to the reduction in mortality for the other major infectious diseases. This graph illustrates the relative contribution of vaccination and antibiotic chemotherapy. By the time these interventions had been introduced, the major infections had already been largely defeated. The question raised by this graph is what really caused the decline in death rates from TB and other infections. We can answer this easily and directly. Firstly, TB did not go away. There is a reasonable chance that a reader is harbouring the disease. Roughly one person in every three in the world (2-3 billion) has the infection. However, only 10-20 million have the active disease. So only one person in every 100 or so infected will have any symptoms. The rest will happily coexist with their "infection" without concern.
http://www.orthomolecular.org/resources/omns/v09n12-graph.jpg People who come down with TB have poor or compromised immune systems. The disadvantaged were living in crowded and damp slum conditions. Although such conditions facilitate spread of the infection this explanation is insufficient. Poor nutrition provides a more direct explanation of why only some of the infected go on to succumb to the illness. TB and Vitamin CDespite the data strongly suggesting the impact of nutrition, corporate medicine has consistently decried the use of supplements. Recently, however, there has been a long overdue development. Catherine Vilchèze and colleagues have returned to testing the extraordinary antibiotic properties of vitamin C for TB.[8] They found that "M. tuberculosis is highly susceptible to killing by vitamin C" [3] which is consistent with previous data. [9] Notably, the mechanism of action is similar to vitamin C's anticancer role in generating hydrogen peroxide locally which kills the unwanted cells. [10] Notably, we have been using antibiotic treatment of TB as a model for the role of vitamin C based redox therapy for cancer. The same mechanism is used to protect the body against both microorganisms and abnormal cancer cells. Supplementation with vitamin C may prevent TB infection from becoming overt. Furthermore, vitamin C could provide an effective biological treatment for TB with the advantage of a mechanism refined by millions of years of evolution. As scientific history demonstrates, good nutrition, particularly vitamins C and D, are likely to be far more effective than antibiotics and vaccination in preventing this and other dangerous infective diseases. Vilcheze's suggests that drugs with a similar mechanism of action to vitamin C might be developed (presumably with great commercial advantage). However, such drugs are an unnatural intervention, and are likely to have unnecessary side-effects while vitamin C is safe. The rather obvious implication of providing high-dose nutritional supplements is once again ignored. If supplementation were to be widely applied, our society may find controlling TB is unexpectedly easy. The recent history of antibiotics is one of misuse leading to microbial resistance. Following Multiple Drug Resistant TB (MDRTB) and eXtensively drug resistant forms (XDRTB) we are now faced with Totally Drug Resistant forms (TDRTB). The increasingly ineffective antibiotics have helped promote the return to study vitamin C as a potential treatment. However, we may be faced with something far more threatening. The history of antibiotic abuse is not reassuring. It may be possible to generate more virulent forms despite Vilcheze's confirmation that resistance to vitamin C is exceptionally difficult to induce. The use of drugs with a similar mechanism to vitamin C may lead to resistance to our basic biological defence mechanisms. In other words, corporate misuse of this latest development could return us to the dark days of uncontrolled infections when TB was killing 1 in 4 people in the developed nations. ConclusionMuch of the recent freedom from deadly infectious disease reflects historical improvements in nutrition. Over time the mechanisms by which nutrients help people be more resistant to infections are being elucidated. Increased levels of vitamin D may have provided a lower risk of TB and other infections as well as the deficiency disease rickets. It now appears that vitamin C is "extraordinarily" effective in killing the TB microorganism. Importantly vitamin C kills TB in essentially the same way as it destroys cancer cells. Linus Pauling, Robert Cathcart and others may have been prescient in suggesting vitamin C provides a unique way of maintaining good health. For further reading:To access forty years of articles describing orthomolecular approaches to health management and treatment of disease visit http://orthomolecular.org/library/jom/ References:1. Hobday R.A. (1997) Sunlight therapy and solar architecture, Med Hist, 41(4), 455-472. 2. Koh G.C. Hawthorne G. Turner A.M. Kunst H. Dedicoat M. (2012) Tuberculosis incidence correlates with sunshine: an ecological 28-year time series study, PLoS One, 8(3), e57752. 3. Liu P.T. Stenger S. Tang D.H. Modlin R.L. (2007) Cutting edge: vitamin D-mediated human antimicrobial activity against Mycobacterium tuberculosis is dependent on the induction of cathelicidin, J Immunol, 179(4), 2060-2063. 4. Sato S. Tanino Y. Saito J. Nikaido T. Inokoshi Y. Fukuhara A. Fukuhara N. Wang X. Ishida T. Munakata M. (2012) The relationship between 25-hydroxyvitamin D levels and treatment course of pulmonary tuberculosis, Respir Investig, 50(2), 40-45. 5. Coussens A.K. Wilkinson R.J. Hanifa Y. Nikolayevskyy V. Elkington P.T. Islam K. Timms P.M. Venton T.R. Bothamley G.H. Packe G.E. Darmalingam M. Davidson R.N. Milburn H.J. Baker L.V. Barker R.D. Mein C.A. Bhaw-Rosun L. Nuamah R. Young D.B. Drobniewski F.A. Griffiths C.J. Martineau A.R. (2012) Vitamin D accelerates resolution of inflammatory responses during tuberculosis treatment, Proc Natl Acad Sci U S A, 109(38),15449-15454. 6. Mörner K.A.H. (2005) Nobel Prize in Physiology or Medicine 1905, Presentation Speech, www.nobelprize.org/nobel_prizes/medicine/laureates/1905/press.html. 7. McKeown T. (1979) The Role Of Medicine, Blackwell. 8. Vilchèze C. Hartman T. Weinrick B. Jacobs W.R. (2013) Mycobacterium tuberculosis is extraordinarily sensitive to killing by a vitamin C-induced Fenton reaction, Nature Communications, doi:10.1038/ncomms2898. 9. Hickey S. Saul A.W. (2008) Vitamin C: The Real Story, the Remarkable and Controversial Healing Factor, Basic Health. 10. Hickey S. Roberts H. (2013) Vitamin C and cancer: is there a role for oral vitamin C? JOM, 28(1), 33-46. Nutritional Medicine is Orthomolecular MedicineOrthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org Find a DoctorTo locate an orthomolecular physician near you: http://orthomolecular.org/resources/omns/v06n09.shtml The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource. Editorial Review Board:Ian Brighthope, M.D. (Australia)
Andrew W. Saul, Ph.D. (USA), Editor and contact person. Email: omns@orthomolecular.org This is a comments-only address; OMNS is unable to respond to individual reader emails. However, readers are encouraged to write in with their viewpoints. Reader comments become the property of OMNS and may or may not be used for publication. To Subscribe at no charge: http://www.orthomolecular.org/subscribe.html To Unsubscribe from this list: http://www.orthomolecular.org/unsubscribe.html |

This website is managed by Riordan Clinic
Information on Orthomolecular.org is provided for educational purposes only. It is not intended as medical advice.
A Non-profit 501(c)(3) Medical, Research and Educational Organization
3100 North Hillside Avenue, Wichita, KS 67219 USA
Phone: 316-682-3100; Fax: 316-682-5054
© (Riordan Clinic) 2004 - 2017
Consult your orthomolecular health care professional for individual guidance on specific health problems.