|
|
|
|
Muscular Dystrophy and Nutrition Therapy |

|
|
|
One reader says: "At our sons last visit to the pediatrician, the doctor was completely amazed at how well he is doing. He shows no signs of typical MD that she was expecting based on her experience with conventional medicine." Another reader writes: "I was diagnosed with the FSHD form of muscular dystrophy some years ago and given the typical 'there is no known cure' comment from the muscle specialist, neurosurgeon and my family doctor. I accepted the situation, but continued to hope for some development in the disease. I came across your web site, and read the article on M.D. For the first time in years I felt encouraged and began to try a combination of the items listed in the article. I noticed an immediate increase in my energy level, which felt good in itself, but the "amazing" happened just recently when both my wife and I noticed a increase in the size of my left leg's calf muscle (this is without exercising). It was very obvious. I am continuing with the vitamins and supplements with an eager, though cautious 'one day at a time,' expectation of further results."
by Andrew W. Saul
Important note: I am not a physician and am certainly not a neurologist. Over the years, I have received reports from parents who have noticed two things when they supplement their children's diet with high doses of nutrients: 1) immediately improved quality of life, and 2) a significant delay in symptom progression. That is not cure; that is experience worth sharing.
Everybody knows what
muscles are, and when they dont work, the weakness, frailty and incapacity
of a little child with muscular dystrophy makes for many a poignant poster
and tearful telethon. "There is no treatment
there is no specific
therapy," says the Merck Manual. The National Institutes of Heath
says the same thing: "There is no specific treatment for any of the
forms of MD."
Such despairing,
autocratic but research-friendly pronouncements must not be seen as the last
word until we adequately weigh in fetal malnutrition as a
fundamental cause of muscular dystrophy. The good news (to be considered
further below) is that if nutrient deficiency can cause an illness, nutrient
therapy may ameliorate, or even cure, that illness.
Malnutrition causes
muscular dystrophy? The short answer is, Yes. "Dystrophy: 1. Defective
nutrition. 2. Any disorder caused by defective nutrition." (American Heritage Dictionary of the
English Language, p 407.) When we consider all this means, we are poised
to head down a steep slope. Nothing gets you into the emotional soup faster
than being perceived as blaming a babys problem on the mothers diet.
Truly, it is very difficult to know for sure if a birth defect is the result
of genetics or environmental factors. The mother represents half of a
developing babys heredity, but almost all of the developing babys
environment. Every single cell in a baby is the product of inherited DNA
instruction. But every single cell in a baby is also the product of the
mother's diet.
"Dinner Table
Heredity"
Ova (human eggs) are
formed during the fetal stage of a females life. In other words, all of a
womans own eggs are actually formed while she was developing inside her
mother, before she herself was born. Wow. This means that what your
grandmother ate significantly contributed to your anatomy. Think that one
over: What looks to be purely a genetic problem may in fact be a largely a
nutritional one. I call this "Dinner Table Heredity." Just because
a problem comes out of the womb does not mean that that problem is genetic
and only genetic. Science has known for decades that many a specific birth
defect is a direct result of a specific vitamin deficiency. (1-3)
Spina bifida, now
well-known to be caused by a lack of folic acid (folate), is an example. I
personally was born with a slight degree of spina bifida. I do not blame my
mother; I might blame those who wrongly advised her about her pregnancy diet.
I most certainly blame the food processing industry for systematically milling
away the B-complex vitamins from her daily bread, and I blame the government
for letting them get away with it.
Unlike spina bifida,
muscular dystrophy may be reversible. However, MD is almost certainly not a matter of
simple malnutrition, for it often does not respond to low-dose nutrient
therapy. But it may sometimes respond to high-dose nutrient therapy, and may therefore
be what orthomolecular physicians call a "genetotrophic" disease.
GENETOTROPHICS
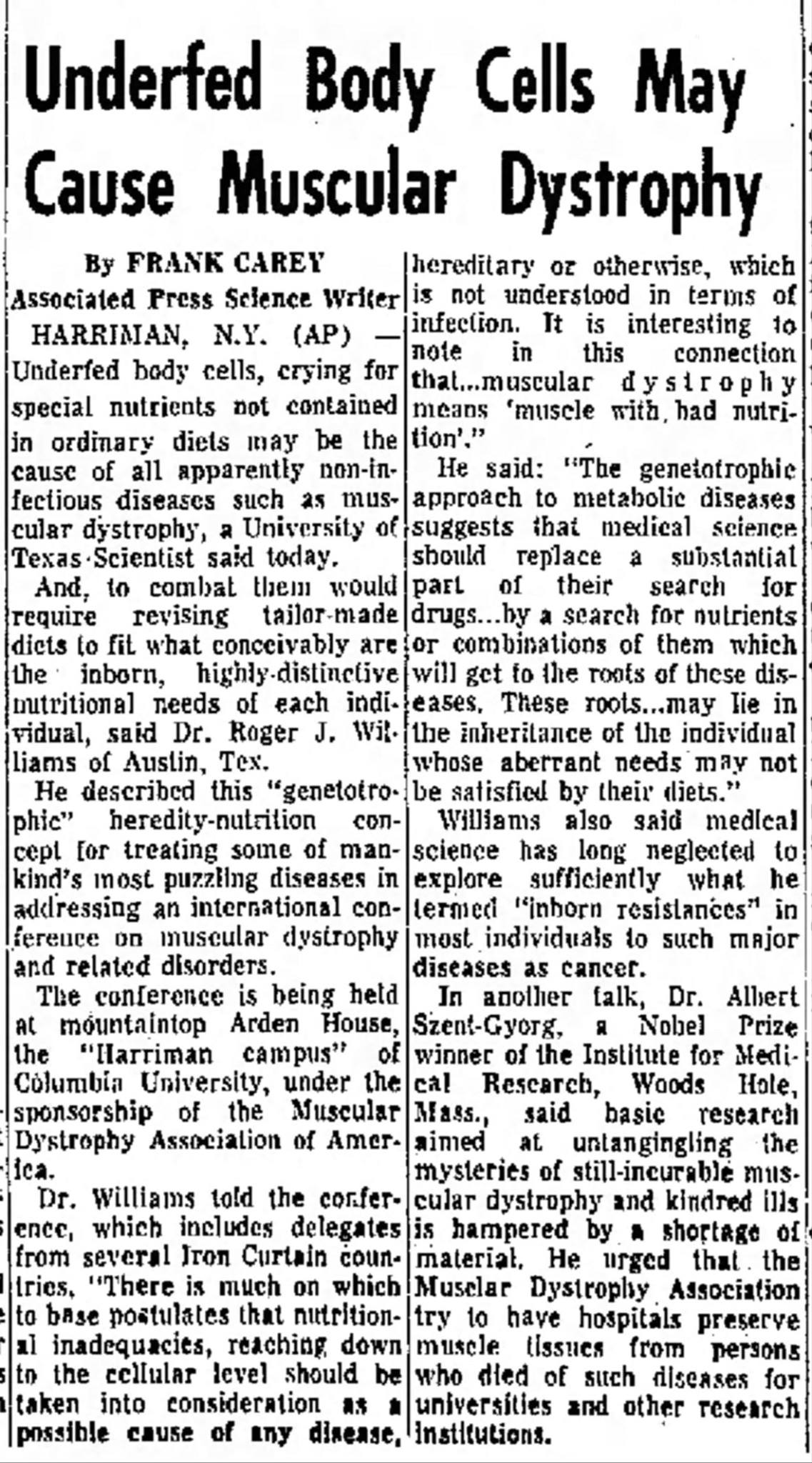
The important
interrelationship between food and the genes was first called the
"genetotrophic concept" by Roger J. Williams, PhD. Dr. Williams,
the discoverer of the B-vitamin pantothenic acid, has explained in his books
and scientific papers how existing biochemical birth defects may be
effectively overcome with optimum nutrition. (http://www.doctoryourself.com/biblio_williams.html). Please consider (and note the
publication date):
Williams RJ. (1953).
Muscular dystrophy and individual metabolic patterns: The possibilities of a
nutritional therapeutic approach. Proc. of the First and Second Medical
Conferences [1951-1952] of the Muscular Dystrophy Assoc. of America, 118-22
(Additional references below, 4-7.)
In genetotrophic diseases, genetic abnormality leads to
nutritional disability. To compensate, the body requires the availability of larger than
normal quantities of one or more nutrients for the affected gene to
successfully express itself. For that particular person, normal dietary
vitamin intakes are quite inadequate for normal function. It is a bit like
trying to take a hot bath with the drain open: it can be done, but you are
going to need a lot more hot water.
I think muscular
dystrophy may constitute a good example of a genetotrophic disease. This also
goes a long way to answering the perennial parents' question as to how one
child can be healthy while the sibling is afflicted with MD. . . when Mom ate
pretty much the same diet during both pregnancies. There may be both a
genetic component and a nutritional component. Rather than a nutrient
deficiency, MD may more exactly be
considered to be a genetically-influenced nutrient dependency.
IS THERE A WAY OUT?
To a family with a child
with muscular dystrophy, it must seem like the worst form of Monday morning
quarterbacking to say what might have caused the disease their child already
has. So the real question is, To what extent might
individual nutrients enable the sufferer to overcome the existing condition?
There is considerable good news, and all of it is nutritional.
COENZYME Q10
By now, CoQ10
(umbiquinone) should probably be accepted as a vitamin. Many other vitamins
are coenzymes. CoQ10 is found in very tiny quantities in foods. Most young
people make CoQ10 in their bodies, but a youngster with muscular dystrophy
may either make too little or have a bigger requirement because of the illness.
It has been established
that heart muscle greatly benefits from CoQ10 supplementation, resulting in
improvement in cases of congestive heart failure and even cardiomyopathy.
Striated cardiac muscle and striated voluntary (skeletal) muscle are not that
dissimilar. Furthermore, Folkers et all write that:
"Cardiac disease is commonly associated with
virtually every form of muscular dystrophy and myopathy. . . The rationale of
this trial was based on known mitochondrial myopathies, which involve
respiratory enzymes, the known presence of CoQ10 in respiration, and prior
clinical data on CoQ10 and dystrophy. These results indicate that the
impaired myocardial function of such patients with muscular disease may have
some association with impaired function of skeletal muscle, both of which may
be improved by CoQ10 therapy. . . CoQ10 is the only known substance that
offers a safe and improved quality of life for such patients having muscle
disease." (8)
Because CoQ10 is so
absolutely vital to muscle cells, involved with growth control, cellular
energy production, and other essential life functions, it warrants special
consideration for persons with muscular dystrophy.
In two
placebo-controlled, double-blind trials, 100 mg CoQ10 daily resulted in
"definitely improved physical performance" in patients with
muscular dystrophies and atrophies. "In retrospect," the authors
wrote, "a dosage of 100 mg was too low although effective and
safe." But even at this low dose, their conclusion was emphatic:
"Patients suffering from these muscle dystrophies and the like should be
treated with vitamin Q10 indefinitely." (9)
I submit that 300-600
mg/day of CoQ10 would be a more effective dose, especially for an older MD child. For most
families, the limiting factors will be cost or medical disapproval. Even
pricey supplements are cheaper than most drugs. And as there are no harmful
side effects with CoQ10, it is inexcusable to NOT give it a serious
therapeutic trial.
Let's be fair: If CoQ10
is important to rabbits, might it also be important to children? (Boler JB,
Farley TM, Scholler J, Folkers K. Deficiency of coenzyme Q10 in the rabbit.
Int Z Vitaminforsch. 1969;39(3):281-8.)
VITAMIN E
Like CoQ10, vitamin E is
an antioxidant. There is a long history of scientific suspicion, to this day
largely untested, that antioxidants are of unusual benefit to individuals
with muscular dystrophy. Linus Pauling wrote about muscular dystrophy, both
experimental and hereditary, in How to Live
Longer and Feel Better. Dr. Paulings comments are here reprinted with
permission of the Linus Pauling Institute,
"It was
recognized more than fifty years ago that a low intake of E leads to muscular
dystrophy, a disorder of the skeletal muscles characterized by weakness
similar to that caused by a deficiency of vitamin C (the studies of vitamin E
and muscular dystrophy have been discussed by Pappenheimer; 1948). . .
Several kinds of hereditary muscular dystrophies are known. For the most part
their nature is not thoroughly understood, and there is no specific therapy
recommended for them. Myasthenia gravis is treated by inhibitors of
cholinesterase, corticosteroids, and surgical removal of the thymus gland.
The medical authorities do not mention the possible value of vitamins in
controlling muscular dystrophies. The evidence about the involvement of
vitamin E and vitamin C as well as B6 and other vitamins in the functioning
of muscles suggests that the optimum intakes of these nutrients should be of
value to the patients. So far as I know, no careful study of an increased
vitamin intake for patients with hereditary muscular dystrophy has been
reported." (p
160)
With the exception of the
CoQ10 studies referenced above, Dr. Pauling's statement of 20 years ago,
unfortunately, still pretty much stands. I found a couple of studies, one
with 15 patients using vitamin E and selenium reporting "minimal"
benefits (10) and another with 16 patients, showing "slight" benefit
(11). I think they would have obtained far better results if they had used
larger doses of selenium, much larger doses of vitamin E, and only the
natural form of vitamin E.
Then there was this
study, using 600 mg of vitamin E and a high amount of selenium (4,000 mcg
Na2SeO3), which got very good results in all five patients studied. "All improved their grip strength. . ., two normalized their
gait, another two can now sit down on their heels and stand up, one patient
can now walk on his toes, one can now get up from lying on the floor without
using a chair and two patients have improved their physical capacity. . . No
side-effects were observed." (12)
This is, at the very
least, genuinely encouraging.
Why no new, large-scale
studies of high dose selenium-vitamin E therapy? Because drugless therapy is
ignored by drug companies, and consequently remains unpromoted and unknown to
physicians. There is no money in products that cannot be patented. Children
learn at an early age that mud pies don't sell. No investment is made, no
research is done where there is no money is to be recovered. Drug companies
do not expect to find, nor do they want to find, a cure that does not involve
a drug. A tragic example is modern medicine's approach to muscular dystrophy.
No doubt Jerry Lewis was a
great guy and his heart was in the right place. Yet telethons to raise cash
for drug research for muscular dystrophy are expensive anachronisms. They are
just re-inventing the wheel, and they're building it wrong to boot. Remember:
"Dystrophy" means "malnutrition." There is no drug that
corrects malnutrition, and never will be.
Agricultural scientists
know this. You will have little
trouble finding research studies on the role of selenium or vitamin E in
preventing muscular dystrophies in chickens, cattle or calves, sheep or
lambs. What works with calves should, in my opinion, be reasonably
applied to people. (13,14)
Yet in spite of the long
and expensive history of research on human muscular dystrophy, only a very
small portion has involved vitamins, and was done quite some time ago. In the third edition of The Vitamins in Medicine,
Bicknell and Prescott provide a thorough review of the literature on pages
612-619 and 635-641. There is considerable evidence that the disease is an
inability of muscle tissue to efficiently utilize vitamin E. I give you the
following quote: Synthetic vitamin E will not work. On pages 643-644 of The Vitamins
in Medicine, DL alpha tocopherol (synthetic "vitamin E") is
described as "valueless." It has to be the natural
"D-alpha" form, specifically including the complete mix of natural
tocopherols and tocotrienols, preferably from or with fresh stone ground
whole wheat bread, wheat germ, or wheat germ oil. (p 645).
Muscular dystrophy is
described as easier to cure in children, and easier still with added B vitamins
and vitamin C (p 644).
Perhaps the most
remarkable revelation of all is that this medical textbook was written in 1953. Has the human body changed in
55 years? Has muscular dystrophy changed in 55 years? No. Only our understanding of a disease can be said
to have changed, and in this case, has changed for the worse. We have ignored
the evidence, and doctors still tell patients that MD is incurable. If that
angers you, read on.
SELENIUM Blood levels of selenium
are reduced in muscular dystrophy. "Myotonic dystrophy and all its major
symptoms (including muscle dystrophy) can be cured or prevented in animals by
selenium supplementation." (Werbach M. (1988) Nutritional Influences
on Illness,
The vitamin-E-friendly
mineral selenium is found in nutritional (or brewers) yeast, seafood,
legumes, whole grains, animal products, and vegetables. However, food can be
an unreliable source of selenium, as selenium content of soils varies around
the nation.
For normally healthy
individuals, overdose of selenium is possible with chronic excessive dietary
intake. But we need to bear in mind that in the Orndahl study cited above,
muscular dystrophy patients showed improvement with a daily dose of up to
1,400 mcg elemental selenium over period of nearly two years. Toxicity is
clearly not a major issue.
LECITHIN
Lecithin has been shown
to improve therapeutic response when included along with vitamin E
supplementation. This is probably due to the fact that lecithin contains a
great deal of both inositol and phosphatidvl choline, which appear to reduce
creatinuria in those with muscular dystrophy. Daily dosage used is about 20
g, which is about three tablespoons
per day (15-17).
CONCLUSION A
mother writes:
My child
will be two later this month. He was labeled with muscular dystrophy (MD)
last year, quite by accident. He had an issue with breath holding: he held
his breath at daycare too long, passed out, and they called an ambulance. He
ended up in the hospital for seven days of testing, and at the end of those
tests is when they tested for MD.
I was
told by the muscular dystrophy doctor that his life expectancy will be a
wheelchair by 10 years old, and death by 20 years old. As you can
understand, it was quite a shock to our family. The following weeks
later, when the DNA tests came back as positive for either Duchanes or
Beckers MD, I was totally confused. Our pediatrician told us that the
medical world doesnt really know with the DNA testing what type
that will
be determined as he develops, but since he had been diagnosed so early,
it was most likely Duchanes, and she was very sorry that there was nothing
that could be done.
The one
thing that we did take away from the hospital experience as well as then the
initial discussions with our pediatrician, was that once he had been given
the MD label, people started treating him as a label, and not as a
person. This experience has prompted us to not tell many people (unless
its needed) of the label he has been given, as we want people to see the lad
first as the person he is.
My
husband and I (with extended family support) decided this was not enough. We
were not willing to accept that there is simply nothing we could do. Fortunately
for us we found the DoctorYourself website by searching MD and nutrition on
the internet.
The
following are the supplements that our child, age two, currently takes, and
has been for the past year. He is now 33 inches tall and weighs 25 lbs.
Daily:
Liquid
childrens multivitamin (daily serving)
Liquid
Calcium (600 mg)
Liquid
Vitamin E (150 i.u.)
Cod Liver
Oil (daily serving)
Soy Lecithin
(1-2 tsp)
Flax
seeds & wheat germ oil when can get into foods, banana bread, yogurt,
etc.
In
addition, over a two day span, in a powdered form mixed together and put into
milk (I try to do it in equal amounts over each day)
1,000 mg
Taurine
400 mcg
folic acid
60 mg CoQ10
50 mcg
selenium
1,000 mcg
Vitamin B12
1,000 mg
Vitamin C
120 mg
Gingko
4,000 mg
MSM
20 g whey
protein
8000 mg
L-Glutamine
1,500 mg
L-Arginine
800 mg
Creatine
Additionally,
we try to ensure a healthy diet, including organic milk products, fruit and
vegetables, and limit refined sugar in his diet (but certainly do no limit it
completely just try to use info from Dr. Sauls website on healthy eating
for children). We do other non-nutritional things too, including seeing
a physical therapist twice a month.
At our
sons last visit to the pediatrician, the doctor was completely amazed at how
well he is doing. He shows no signs of typical MD that she was expecting
based on her experience with conventional medicine. While this is admittedly a long way from cure, I think it is very encouraging. There is little if any downside to trying nutritional therapy. Bad nutrition has never improved anything, and good nutrition frequently has.
REFERENCES:
1. Hillemann HH. (1956)
"Maternal Malnutrition and Fetal Prenatal Development Malformation"
(Address at
2. Hillemann HH. (1958)
"Maternal Malnutrition and Congenital Deformity" (
3. Hillemann HH. (1961)
"The Spectrum of Congenital Defect, Experimental and Clinical" Journal of Applied Nutrition 14:1,2.)
4. Williams RJ.
Beerstecher E, Jr, and
5. Williams RJ.
"Concept of Genetotrophic Disease," Nut. Rev, 8, 257-60 (1950).
6. Williams RJ. "The
Unexplored Field of Genetotrophic Disease," MD, 6, 123-4, 136 (1951).
7. Williams RJ. and
Rogers, LL. "The Formulation of a Genetotrophic Supplement for the
Experimental Treatment of Diseases of Obscure Etiology,"
8. Folkers K, Wolaniuk J,
Simonsen R, Morishita M, Vadhanavikit S. Biochemical rationale and the
cardiac response of patients with muscle disease to therapy with coenzyme
Q10. Proc Natl Acad Sci U S A. 1985
Jul;82(13):4513-6.
9. Folkers K, Simonsen R
(1995) Two successful double-blind trials with coenzyme Q10 (vitamin Q10) on
muscular dystrophies and neurogenic atrophies. Biochim Biophys Acta 1271(1):281-6. May 24.
10. Backman E, Henriksson
KG. Effect of sodium selenite and vitamin E treatment in myotonic dystrophy. J Intern Med. 1990 Dec;228(6):577-81.
11. Gamstorp I, Gustavson
KH, Hellstrom O, Nordgren B. J Child
Neurol. 1986 Jul;1(3):211-4. A trial of selenium and vitamin E in boys
with muscular dystrophy.
12. Orndahl G, Sellden U,
Hallin S, Wetterqvist H, Rindby A, Selin E. Myotonic dystrophy treated with
selenium and vitamin E. Acta Med Scand.
1986;219(4):407-14.)
13. Orndahl G et al.
(1983) Selenium therapy of myotonic dystrophy. Acta. Med. Scand. 213:237.
14. Hidiroglou M, Jenkins
K, Carson RB, Brossard GA. Selenium and coenzyme Q10 levels in the tissues of
dystrophic and healthy calves. Can J
Physiol Pharmacol. 1967 May;45(3):568-9.
15. Jackson MJ, Jones DA,
Edwards RH. Vitamin E and muscle diseases. J Inherit Metab Dis. 1985;8 Suppl
1:84-7. (This review explains how vitamin E, and the phospholipids in
lecithin, benefit the muscles.)
16. Milhorat AT and
Bartels WE. (1945) The defect in utilization of tocopherol in progressive
muscular dystrophy. Science 101:93-4.
17. Milhorat AT et al.
(1945). Effect of wheat germ on creatinuria in dermatomyositis and
progressive muscular dystrophy. Proc. Soc. Exp. Biol. Med. 58:40-1.
Copyright 2008, 2007 and
prior years by Andrew W. Saul. Revisions copyright 2019.
Andrew Saul is the author of the books FIRE
YOUR DOCTOR! How to be Independently Healthy (reader reviews athttp://www.doctoryourself.com/review.html
) and DOCTOR YOURSELF: Natural Healing that Works. (reviewed at http://www.doctoryourself.com/saulbooks.html
)
|
|
|
AN IMPORTANT NOTE: This page is not in any way offered as prescription, diagnosis nor treatment for any disease, illness, infirmity or physical condition. Any form of self-treatment or alternative health program necessarily must involve an individual's acceptance of some risk, and no one should assume otherwise. Persons needing medical care should obtain it from a physician. Consult your doctor before making any health decision. Neither the author nor the webmaster has authorized the use of their names or the use of any material contained within in connection with the sale, promotion or advertising of any product or apparatus. Single-copy reproduction for individual, non-commercial use is permitted providing no alterations of content are made, and credit is given. | |
|
|
|
| Home | Order my Books | About the Author | Contact Us | Webmaster | |